This patient presented with ‘dizziness’. An ECG is handed to you.
What is the diagnosis?
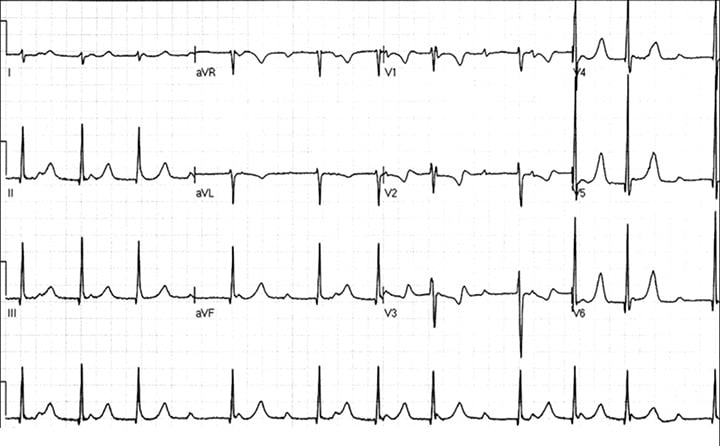
This ECG shows a Type I Wenckebach block
Lets review using the ECG in 20 Seconds approach:
RATE: 11 x 6 = 66bpm
IS IT SINUS?
Are there P waves? and are they inverted in aVR and upright in II? YES
Are the P waves associated with the QRS’s They don’t appear to be. In fact they appear to be disassociated from the QRS….BUT are they? If it were a complete heart block, we would expect a more regular QRS and at probably a slower rate, as it would be coming from the ventricles. Let’s look at the QRS in more detail.
WHAT ABOUT THE QRS’s
They’re not too tall or too small, too wide or too narrow, nor do they have abnormal morphology.
They are clumped together however. When that happens always think of a Mobitz type of block.
WHAT DO WE NEED FOR A MOBITZ BLOCK?
Constant p-p interval, otherwise it may be premature atrial contraction.
We have a constant p-p interval.
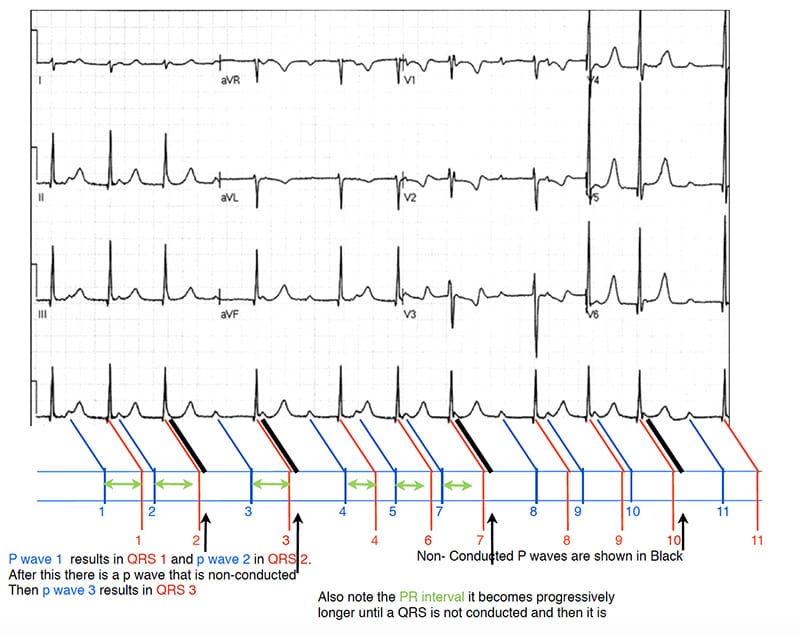
For a Type I second degree block (Wenckebach), there is a PR prolongation until a QRS is dropped. The PR interval right after this is shorter.
For a Type II Mobitz, we need a regular dropping of a QRS and the PR interval stays the same.
P waves generate a QRS and some are not conducted. The diagram below this demonstrates the PR prolongation.