
A 50 year old man presents to the emergency department with shortness of breath and sharp chest pain for the previous 24 hours. There has been no trauma and the patient has no past medical history, on no medications and denies the use of any illicit drugs. This is his ECG: Please make a diagnosis and give an outline of the causes.
Using the ‘ECG in 20 Seconds’ method:
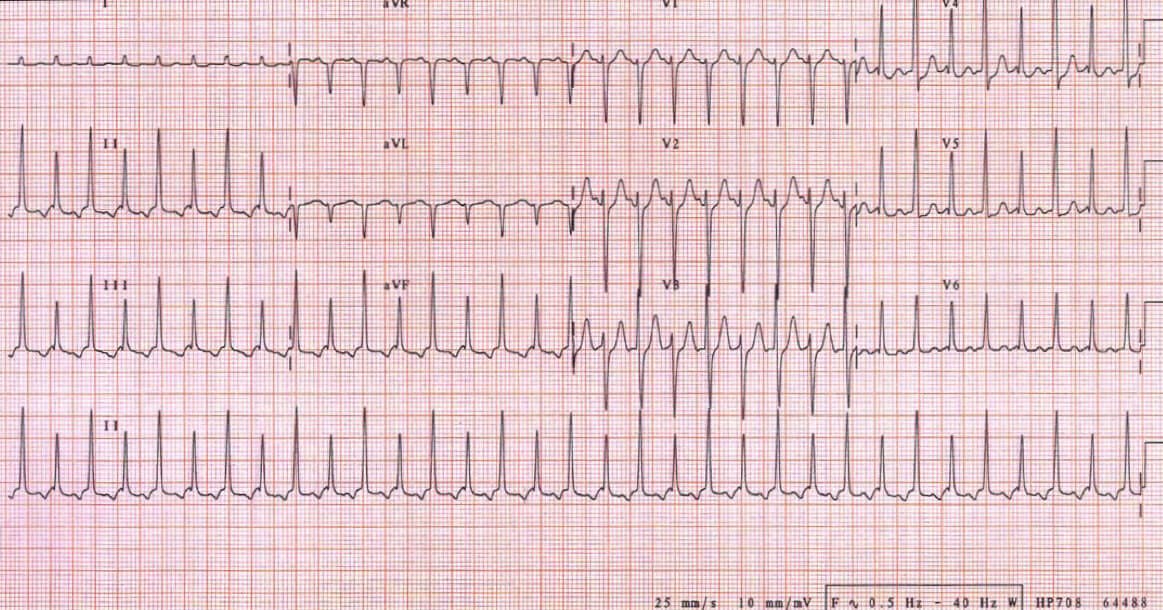
Rate: 25 x 6 = 150 bpm
Rhythm: It is hard to see P waves at this rate, however, I believe that there are P waves in V1 and V5 and II, so I will call this sinus rhythm
QRS: Narrow complexes, borderline left ventricular hypertrophy, with normal morphology(no delta wave), except that the height of the QRS alternates, between high and low. This is ELECTRICAL ALTERNANS.
Axis: Normal
ST-T: There is no evidence of ST elevation, but there is some ST depression evident in lead V4, which is probably rate related. The T waves look a little peaked in V3 and there is T wave inversion in the inferior leads.
PR/QT: PR interval is fine, although the QT interval is prolonged.
The diagnosis is a sinus tachycardia with electrical alternans.
The causes of alternans are several but mainly fall into three categories:
1. Repolarisation: This involves the ST segments and the T wave.
T wave alternans is reported in long QT syndrome(precursor to Torsades) and in electrolyte abnormalities(hypo-Ca,K,Mg). It is also associated with cardiomyopathy or acute pulmonary embolism.
ST alternans is associated with changes in ST segment during ischaemia and is associated with acute myocardial infarction.
2. Conduction alternans: This is the result of a change in impulse propagation
It is seen in myocardial infarction, atrial fibrillation and Wolf Parkinson White syndrome and pulmonary embolism. In the setting of a narrow QRS tachycardia, it may be an orthodromic atrioventricular re-entry tachycardia.
3. Cardiac motion: This is the result of abnormal movement of the heart.
It can be caused by pericardial effusion and hypertrophic cardiomyopathy.
In this patient at 50 years of age and with no previous history and the atypical nature of the pain a pericardial effusion is a probable cause, however, the complexes are large, not dampened by fluid in the sack. Could it be ischaemic? Absolutely. Could it be a repolarisation issue caused by long QT? It could be.
Given that it is a QRS alternans and the normal sized complexes, I would have as my initial diagnosis, pulmonary embolism, followed by myocardial infarction, followed by pericardial effusion.
Even though it is 3rd on my differentials, I can quickly look at the pericardium, by doing a rapid echo with the emergency department ultrasound machine. If this is normal, then the workup continues for a clot or ischaemia.


