
The U wave is an often ignored deflection on the ECG. It is usually < 1mm, upright and has the same polarity(is in the same direction) as the preceding T wave(1). It is usually seen in the anterior leads V2-V3. It may be present in normal individuals and is sometimes ignored…… beware. Here is a quick look at the U wave. I have a new found respect for it.
It was first described by Einthoven in 1903, yet today we still debate the potential mechanisms that cause it. Amongst those are(2):
- Delayed depolarisation of the His-Purkinje System
- Prolonged depolarisation of mid-myocardial cells(M-cells)
- After potentials due to ventricular stretch
The are two things to look for in a U wave:
- It’s polarity(is it up or down?)
- Its size ( how tall is it?)
Polarity of the U wave
The U wave is usually upright and in the same direction as the preceding T wave. A negative U wave is not often seen, but when present, is very specific for heart disease. When present at rest, it may be an early indication of unstable angina or myocardial infarction(3) and may indicate left anterior descending artery disease.
When U waves appear during exertion, they may indicate left circumflex or right coronary artery disease with abundant collaterals(4).
Other causes of inverted U waves include:
- Hypertension
- Congenital Long QT syndrome
- In this case the U wave doesn’t occur after the T wave, but is superimposed on the T wave, interrupting it.
- Left Ventricular enlargement
- Valvular Heart disease(aortic or mitral)
Pre and Post Stent
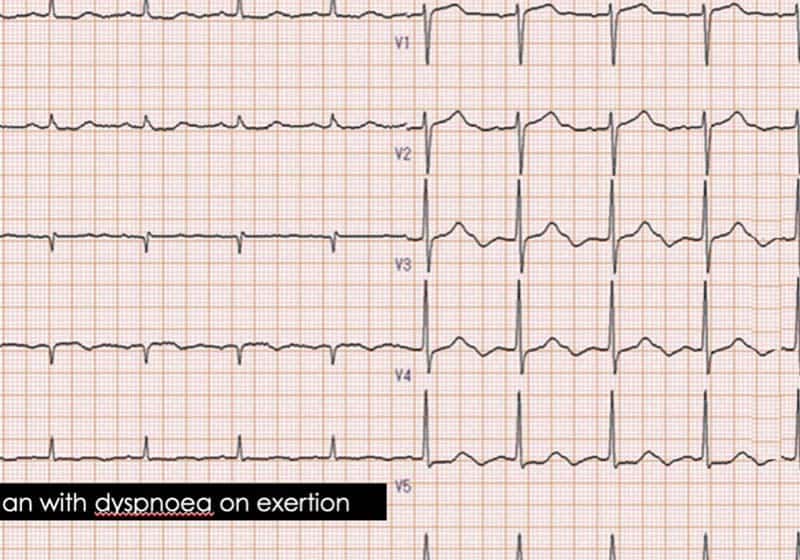
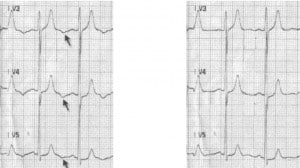
In this case(5), a 50 year old male, chronic smoker, non hypertensive and non diabetic presented with unstable angina. The ECG showed very prominent U waves, but little else.
The coronary angiogram showed a 90% stenosis of the mid left anterior descending artery, which was stented. The U waves resolved post procedure.
The Size of the U wave
The size of the U wave varies inversely with the heart rate, ie., the slower the rate the more prominent the U wave. We therefore expect it to be more prominent in bradycardia. It is usually < 1mm in height and <25% the height of the T wave.
A prominent U wave may be associated with sudden cardiac death(6).
Other causes of a prominent U wave include:
- Hypokalaemia
- Medications
- Class I antiarrhythmics: quinidine, procainamide
- Class III antiarrhythmics: sotalol, amiodarone
- Raised Intracranial pressure
References
- Ariyarajah V et al. Can U waves be “notched”? Ann Noninvasive Electrocardiology. 2008;13(4);426-8
- Correate E et al. The negative U wave: a pathogenic enigma but a useful, often overlooked bedside diagnostic and prognostic clue in ischaemic heart disease. Clin Cardiol 2004;27:674-7.
- Fisch C. The clinical electrocardiogram:sensitivity and specificity. ACC Core J Rev. 1997;6:71-5
- Miwa K et al. Exercise induced U wave alteration as a marker of well-developed and well functioning collateral vessels in patients with effort angina. J Am Coll Cardiol 2000;35:757-63
- Girish MP et al. U wave: An Important Noninvasive Electrocardiographic Diagnostic marker. Ind Pacing and Electrophysiology J 2005;5(1):63-65.
- Was J W et al. Increased U vector magnitude is associated with increased risk of sudden cardiac death- The Atherosclerosis Risk in Communities Study. Circulation 2016;143:A13090
By Peter Kas


