
This is a review of a recent paper in JAMA Cardiology:
Hauw-Berlemont C et al. Emergency vs Delayed Coronary Angiography in Survivors of Out of Hospital Cardiac Arrest. Results of the Randomised, Multicentric EMERGE Trial. JAMA Cardiol. 2022;7(7):700-707. (1)
Our assumption would be that most patients would benefit from coronary angio post survival from cardiac arrest. Let’s put it into context. Our goal is to have neurologically intact survivors.
The authors of this research wanted to determine, if there was any benefit (and which patients might benefit the most) in early coronary angiography in patients with output following out of hospital cardiac arrest if there were no ECG changes consistent with acute infarction.
Previous randomised trials have shown no difference in survival between immediate vs delayed coronary angiography. However registry studies have suggested benefit form early intervention.
A Case
A 72 yo patient normally otherwise well, collapses at home. It is not witnessed, however the patient’s wife is in the next room. She calls the ambulance and commences CPR.
On ambulance arrival, the patient is in PEA, that progresses to Asystole, then PEA again and then a sinus rhythm. He has been treated with 3 doses of Adrenaline.
On arrival to the Emergency Department, he is intubated and has output. His pupils are non reactive and his initial VBG has a pH or 7.12.
What would you rate the chance of good neurological outcome here; low, intermediate or high?
What they did
n=279
Patients were randomised following out of hospital cardiac arrest, with no obvious cause such as trauma, to receive either emergency or delayed coronary angiography.
The Primary Endpoint was 180 day survival, with good neurological outcome.
Secondary endpoints included shock, VT/VF, Survival, and length of hospital stay
Results
There was no difference in overall survival rate with good neurological outcome at 180 days between the two groups (36.2 vs 33.3%)
The study was underpowered.
Why do the Registry Studies results differ?
Firstly, we have seen discrepancies between randomised trials and registry studies in the past.
The selection process in the registry studies may differ, as these patients will undergo selection at the Paramedic and the Emergency level. Decisions about their survival or otherwise are made at those points.
The registry studies found that those with less benefit where those with a higher risk of poor neurological outcome. This might be expected.
Let’s go back yo our case
There are several scoring systems that we can use to determine potential neurological outcome.
One of those is the MIRACLE2 score(2).
The score has some limitations. It was derived from a restrospective chart review. However it determines 7 variables as being important in making predictions on neurological outcome. See below:
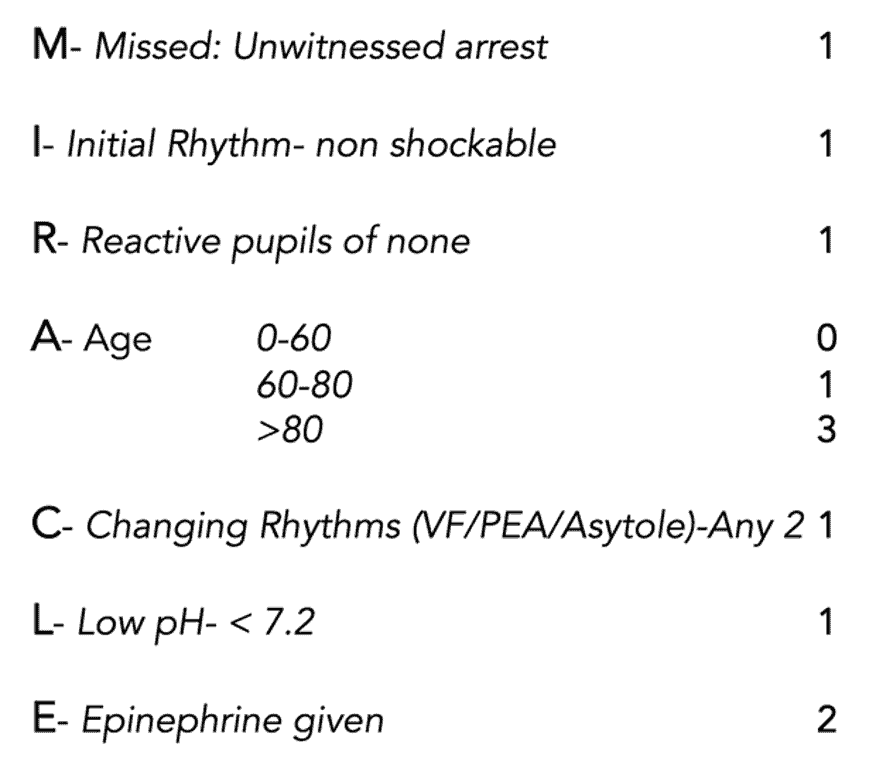
3-4 = Intermediate Risk
>4 = High risk
If we don’t enter a discussion about the utility of pupillary reflex following adrenaline, or acidosis secondary to adrenaline and simply apply the score to our 72 yo patient above.
The score would be a 7/10 ie., a high risk of poor neurological outcome.
At high scores, the positive predictive value of MIRACLE2 is about 92%.
Conclusion
At present we should watch this space. There appears to be no benefit in sending patients to the Cath lab for out of hospital cardiac arrest, if there are no ECG findings of an acute infarction. However younger patients with early CPR and defibrillation, should perhaps still go for early coronary angiography, until we have a better answer.
References
- Hauw-Berlemont C et al. Emergency vs Delayed Coronary Angiography in Survivors of Out of Hospital Cardiac Arrest. Results of the Randomised, Multicentric EMERGE Trial. JAMA Cardiol. 2022;7(7):700-707.
- Pareek N et al. A practical Risk score for early prediction of neurological outcome after out-of-hospital cardiac arrest. MIRACLE2. Eur Heart J. July 2020.


