
Isolated right ventricular infarction is rare, but it does occur in 30-50% of cases of inferior infarction. We need to think of the possibility of right ventricular infarction, or we can miss it.
The right ventricle is thin walled and is perfused throughout the cardiac cycle, explaining why it is less likely to infarct.
It is supplied by the right coronary artery, which also supplies the sinoatrial node and continues to supply the atrioventricular node in a large number of cases. This is the reason that we sometimes see bradycardia and blocks in patients with right coronary artery occlusion.
How do these patients present?
Patients with right ventricular infarction will be pre-load sensitive, due to poor ventricular contractility. The result will be an increase in right ventricular diastolic pressures. Due to being preload dependant, there is a significant risk of severe hypotension when preload is decreased, such as occurs when we give nitrates.
Patients may present with hypotension, clear lung fields and distended neck veins. There may also be unexplained hypoxia, even with high levels of supplemental oxygen. This occurs due to the effects of right to left shunts via patent foramen oval or atrial septal defects becoming more pronounced as right sided pressures increase.
Some patients may present bradycardia due to the right coronary artery supplying the sinoatrial and atrioventricular nodes. These patients can become significantly compromised and require pacing.
Differential Diagnosis
There are many differentials, however some of the more important are:
- Pericarditis
- Cor Pulmonale
- Pulmonary Embolism
- Tricuspid Regurgitation
- Cardiomyopathy
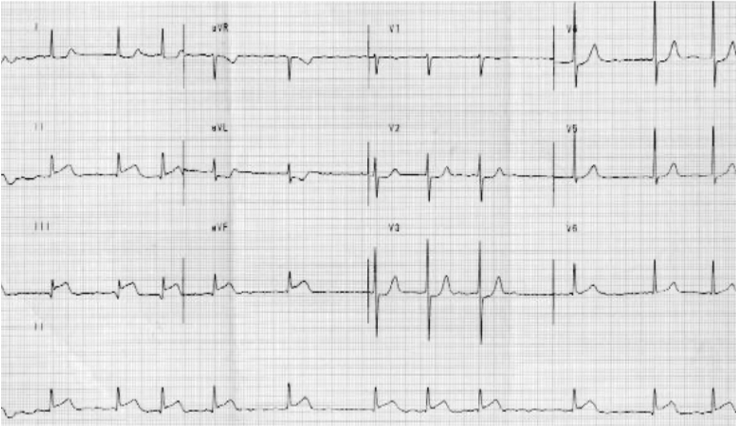
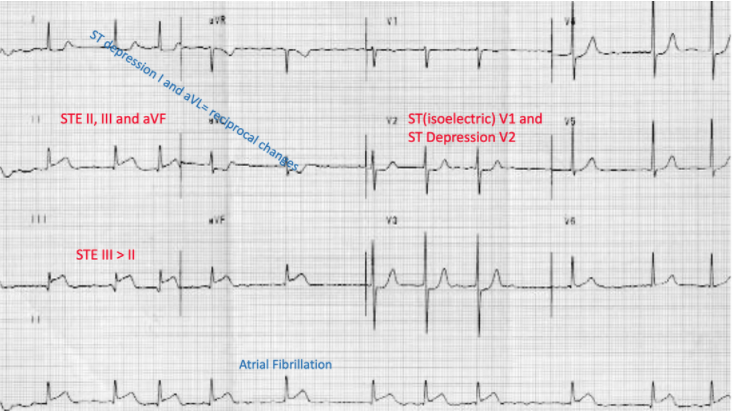
The ECG
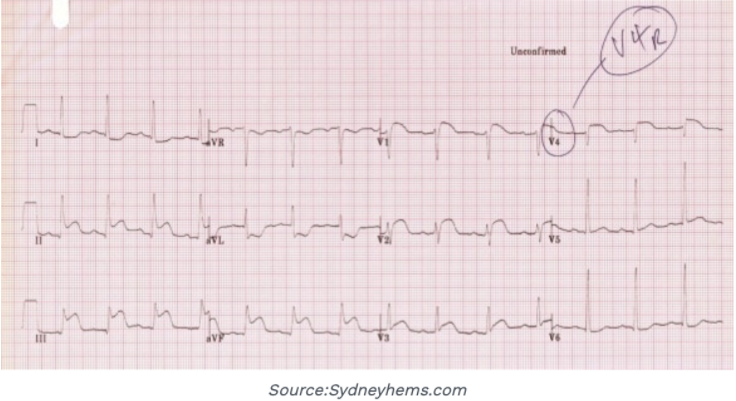
Although echocardiography and other imaging may be required as some point, the ECG is the most important initial investigation, as it can give clues to the diagnosis. Any patient with an inferior infarction needs to have right sided leads. Beware as the right sided ST elevation may be transient.
|
|
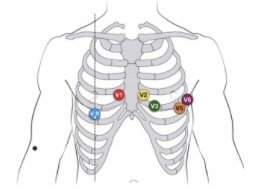
Only one lead needs to be looked at; lead V4R. To record this lead, simply remove lead V4 and place it in the mirror position on the right chest. ST elevation of > 1mm in V4R has an almost 100% sensitivity for right ventricular infarction.
|
Patients with right ventricular infarcts are preload dependent. Start initially with a fluid bolus such as 500ml of crystalloid. This may need to be repeated.
Remember NO NITRATES in pure right ventricular infarction.
If the hypotension continues despite fluid loading consider inotropes. Dobutamine is the drug of choice as it improves cardiac index and right ventricular stroke volume. Remember that this can also decrease blood pressure.
Beware the patient who also has a left ventricular dysfunction. These patients will need support including after load reduction. This can be done with a nitroprusside infusion.


