
I was teaching ‘The ECG in 20 Seconds’ the other day and again thought about how important the lead avR is. Also, how many times had I ignored it and how many times have you?
In the patient that presents with suspected cardiac ischaemia, we should look at the vascular territories on the ECG.
Anterior V1-V4
Lateral V5-V6, I avL
Inferior II, III and avF
We must also look at one other lead, aVR.
This is a very important lead as it can give us information on potential ischaemia in the LMCA, but may also indicate three vessel disease and LAD disease. This is important as most of these lesions will require CABG.
It’s also important, because in the patient with elevation in avR, which may signify a need for CABG, as we have to think; can I give clopidogrel?
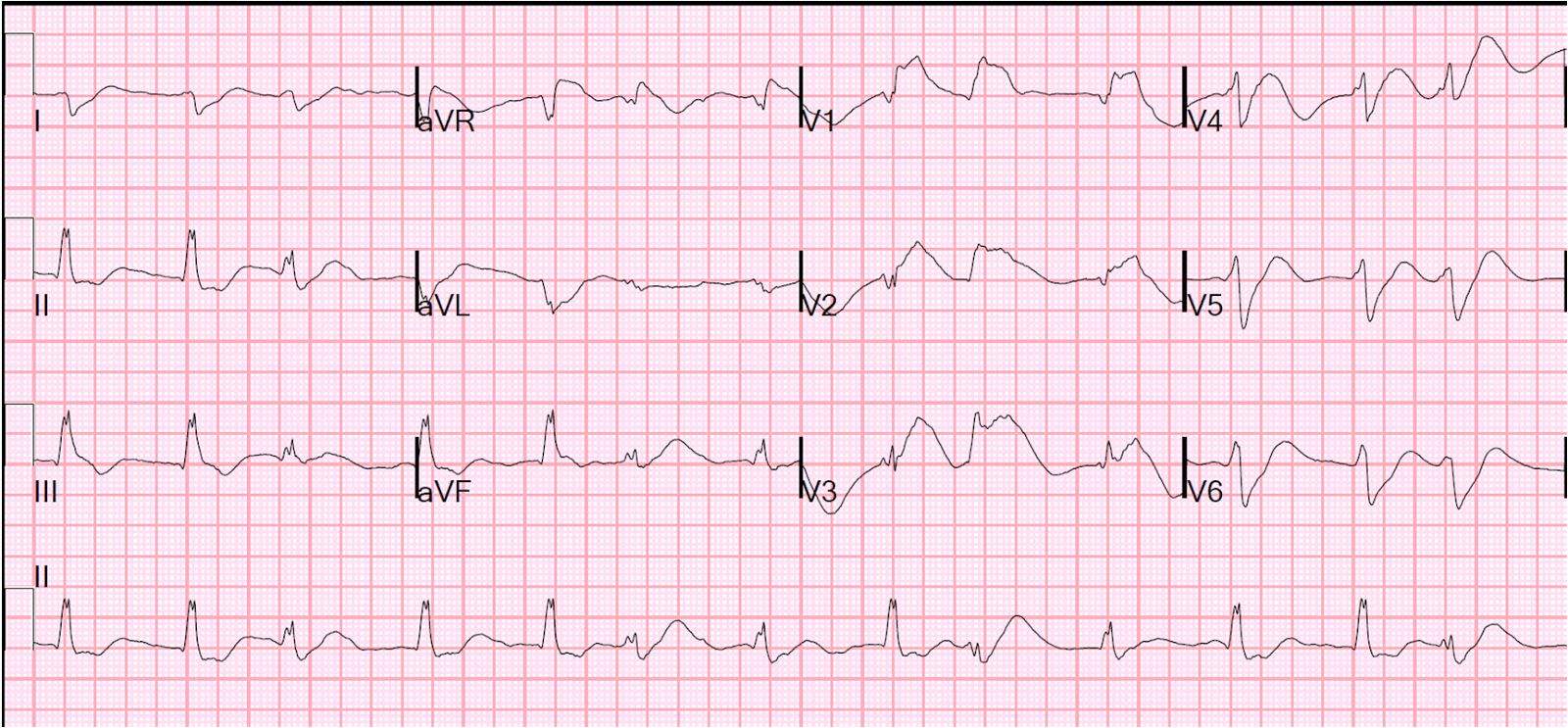
Look at the following ECG and comment:
What we see is ST elevation in avR and a widespread ST depression.
Here are some important points relating to elevation in avR.
- It only applies to those patients with ischaemic symptoms, not as symptomatic patients.
- ST elevation of > 1.5mm is significant
- ST elevation in avR +avL > 95% specific for LMCA obstruction
- avR >V1 = proximal LAD or LMCA occlusion
- ST elevation in avR is normal in SVT
So, don’t ignore this little lead, it’s important.


