
Welcome to the Cardiac Course. This is an online course that has been built from the Cardiac Bootcamp Workshops, which have been attended by just over 2000 doctors, nurses and paramedics and our online cardiac bootcamp. The Course is included in your EM Mastery Membership.
Introduction: The ECG in 20 Seconds Approach
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Module 3. The Paediatric ECG
Paediatric ECG
In this section we look at:
- The Paediatric ECG and How to Read it.
- The differences to know between Adult and Paediatric ECGs
- Paediatric Arrhythmias
- Myocarditis.
Module 4.1 Arrhythmias: Wide Complex Tachycardias
4.0 Arrhythmias
In this section we look at:
- Wide Complex Tachycardias
- Regular
- Irregular
- Narrow Complex Tachycardias
- Atrial Fibrillation and Flutter
- Blocks
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Wide Complex Tachycardia
Here is the GREAT NEWS!
Even if we have no idea, we know that 80% of wide complex tachycardias are Ventricular Tachycardia
Remember these causes of wide complex rhythms:
- Ventricular Tachycardia
- SVT with Aberrancy
- Hyperkalaemia
- Na+ Channel Blockade
- Ischaemia
- Paced Rhythm
If you checked the potassium and knew they hadn’t taken some kind of overdose that block Na+ channels and they had no pacemaker and there was no chest pain and you couldn’t see any ischaemia…..it leaves us with VT and SVT with aberrancy.
Let’s say you were convinced that it was SVT with aberrancy…….Now remember that it would have to be regular ie it were not Atrial fibrillation.
Rules for VT
There are rules that can help us Rule IN VT and Rule IN SVT. There are the rules below as well as others
|
BRUGADA Criteria
Sensitivity of 92% and Specificity of 65% Inconsistent across observers VERECKEI Criteria Similar sensitivity and specificity to Brugada |
So many Things to Look for
There are a lot of things to look for in an ECG when trying to diagnose VT:
1. What is the patient’s age? older= more chance of ischaemia and VT
2. Are the complexes wide? >4 small squares (>160ms)
3. Are there p waves and is there AV dissociation?
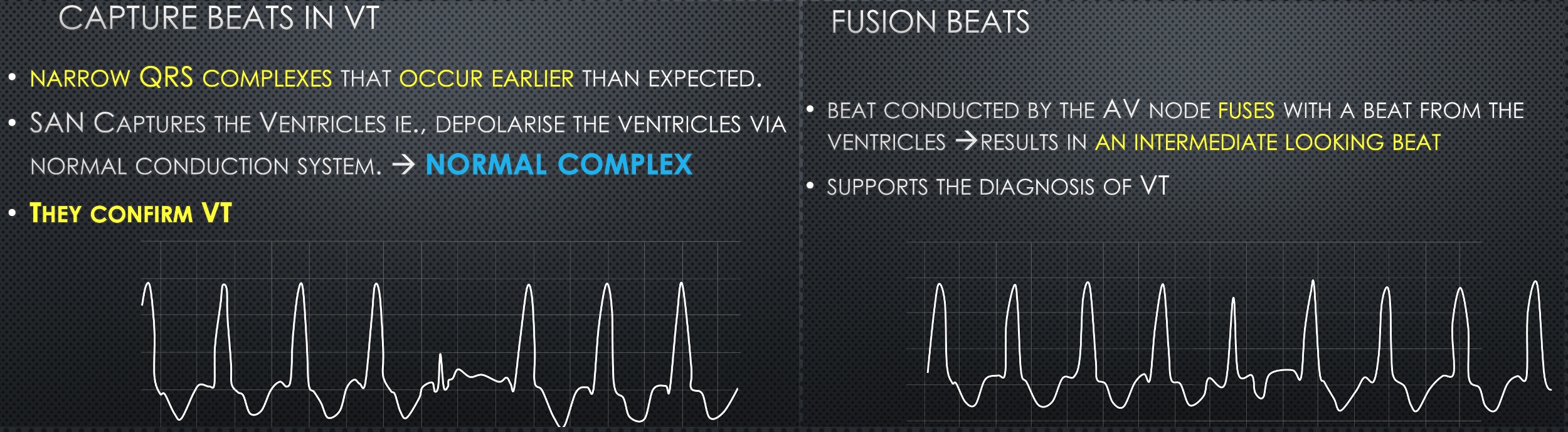
4. Are there Capture beats or Fusion beats
5. Is axis extreme?
6. Is there concordance in V1-V6
7. Is there RSr pattern?
8. Are the signs present
(a)Brugada’s Sign- QRS to S wave > 100ms
(b)Josephson’s Sign-Notching in S wave
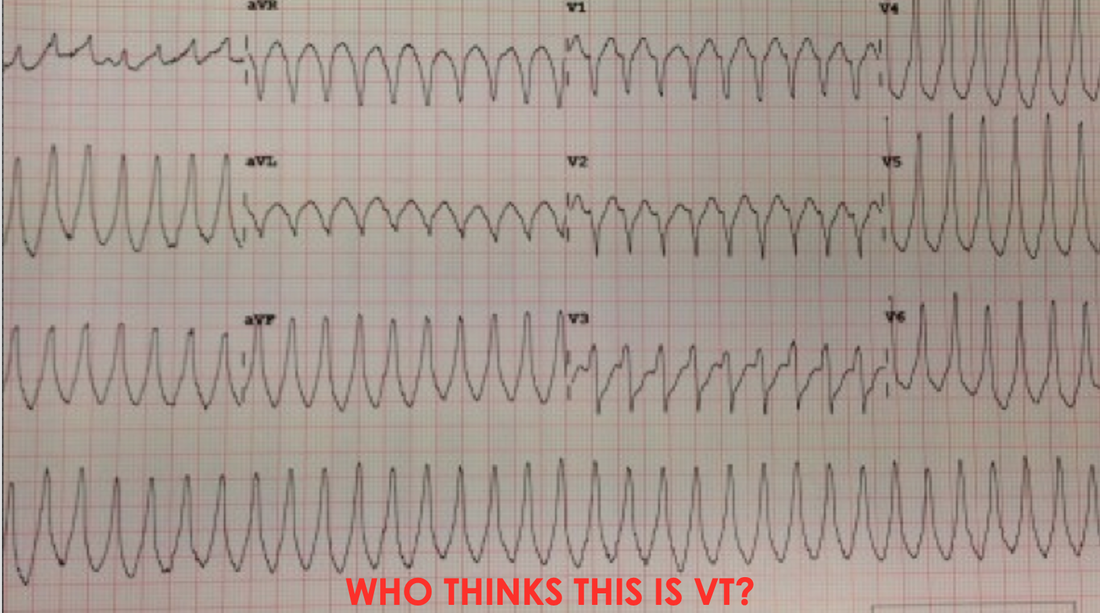
Here’s a Case
A 78 yo male presents to the emergency department with palpitations. He has no chest pain.
His rate is as you see it.
His BP is 110/60.
What is the diagnosis?
IS IT VT?
If you ruled out hyperkalaemia and he hasn’t taken a Na channel blocker and he doesn’t have a pacemaker…. You could if you were convinced that it was SVT(given that it is regular) give adenosine. If it were SVT it would break. if it were VT, it would not.
Case 2


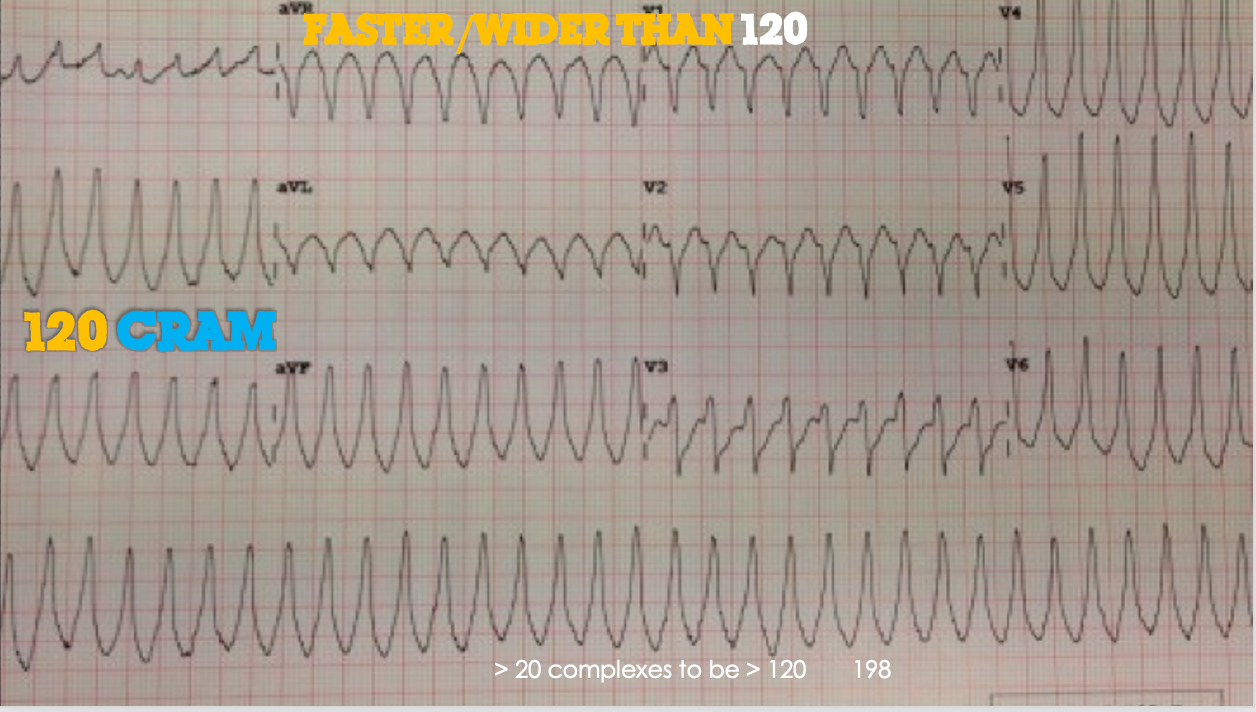
The 120 CRAM Formula for VT
The rule I use to diagnose VT is the 120 CRAM rule
It hasn’t been validated etc, but it’s my personal rule which brings the Brugada and Vereckei together. It may help you.
120 is an important number. “Faster than 120 and wider than 120”
It isn’t VT unless the rate is > 120
The QRS must also be wider than 120ms
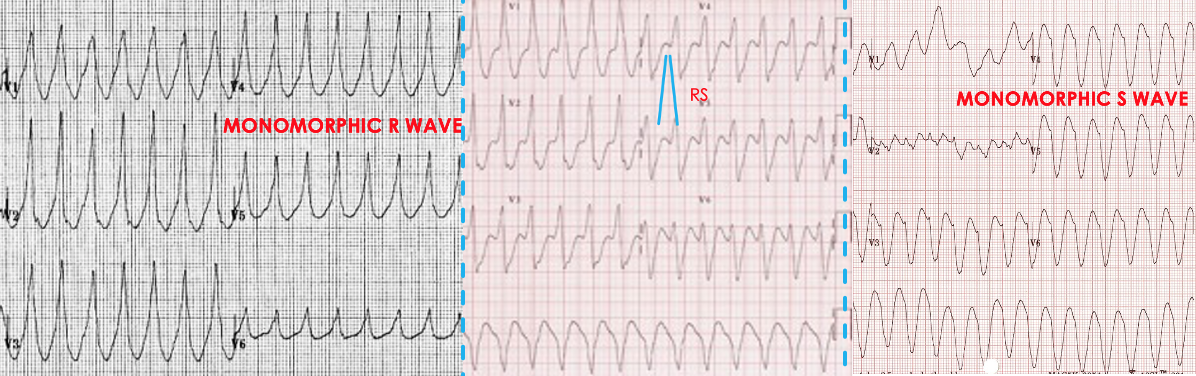
C
Concordance
IF ALL THE PRAECORDIAL LEADS HAVE EITHER:
•A MONOPHASIC R WAVE OR
•A MONOPHASIC S WAVE THEN IT IS VT
R
R Wave in aVR
Is there an initial Dominant R wave in aVR? YES=VT
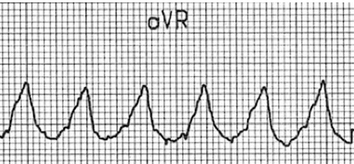
There is a dominant R wave in aVR. This is VT.
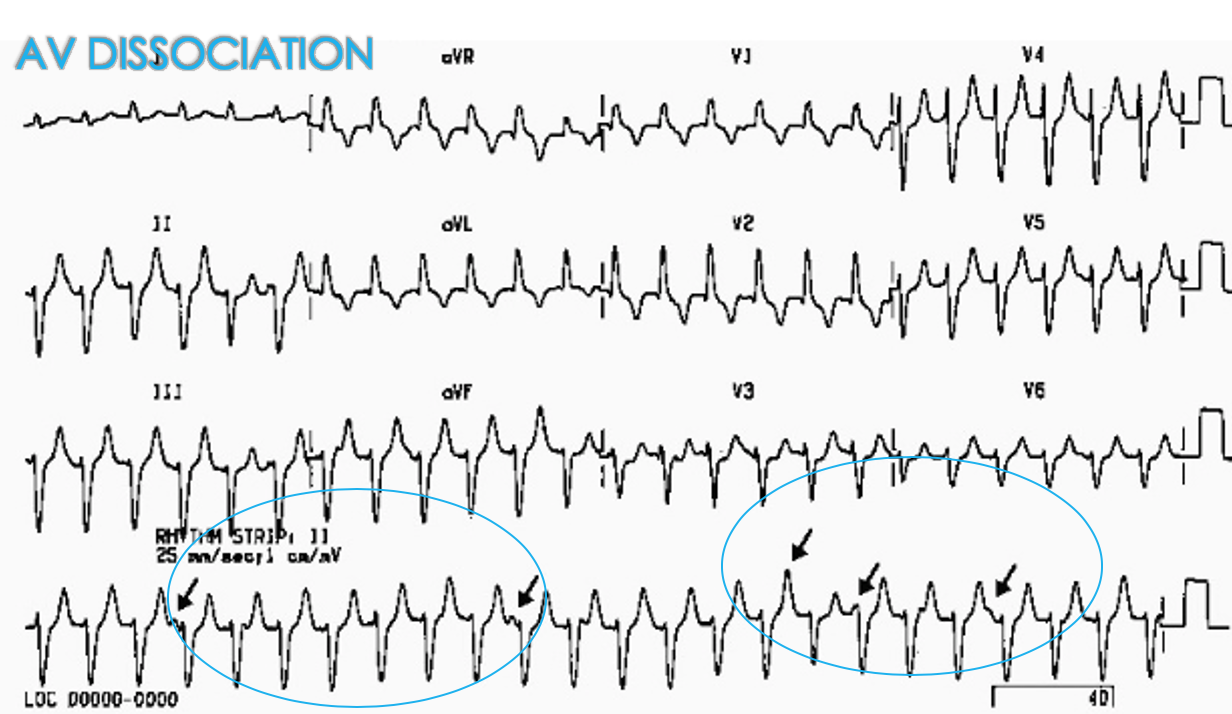
A
AV Dissociation
M
The Morphology: This is the most involved section.
Let’s go over it slowly. You can then follow on the video below.
We are looking for the following:
1.Capture Beats ad Fusion Beats
2. Do the Complexes have a RBB or LBB Morphology?
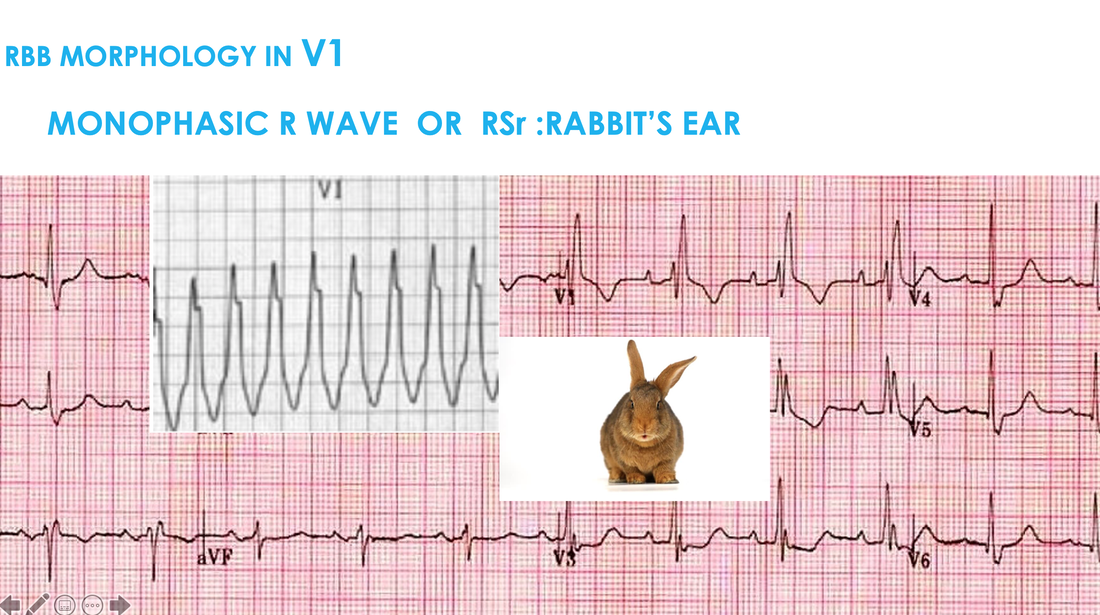
2(a) RBB Morphology
- R wave(V1)
- Right Rabbit Ear(V1)
- qR(v1)
- R/S < 1 in V6
2(b) LBB Morphology
- Notched S wave
- Josephson’s Sign
- Brugada Sign
- qR in V6
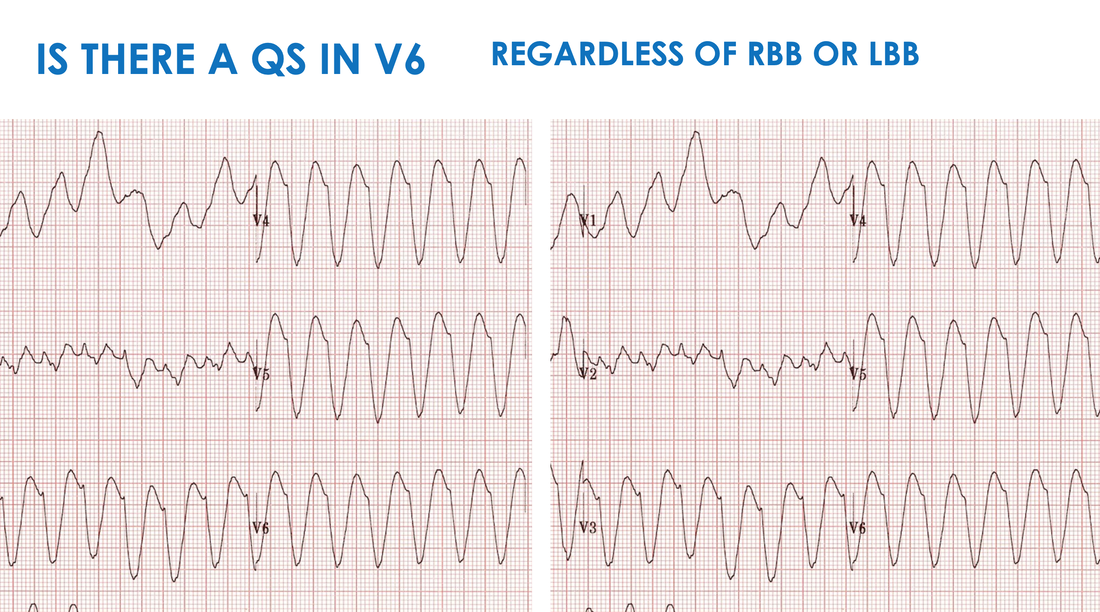
3.Is there a QS in V6?
Let’s look at case 1 and use the 120 CRAM approach
 So it is Faster than 120 and wider than 120 and it looks real.
So it is Faster than 120 and wider than 120 and it looks real.
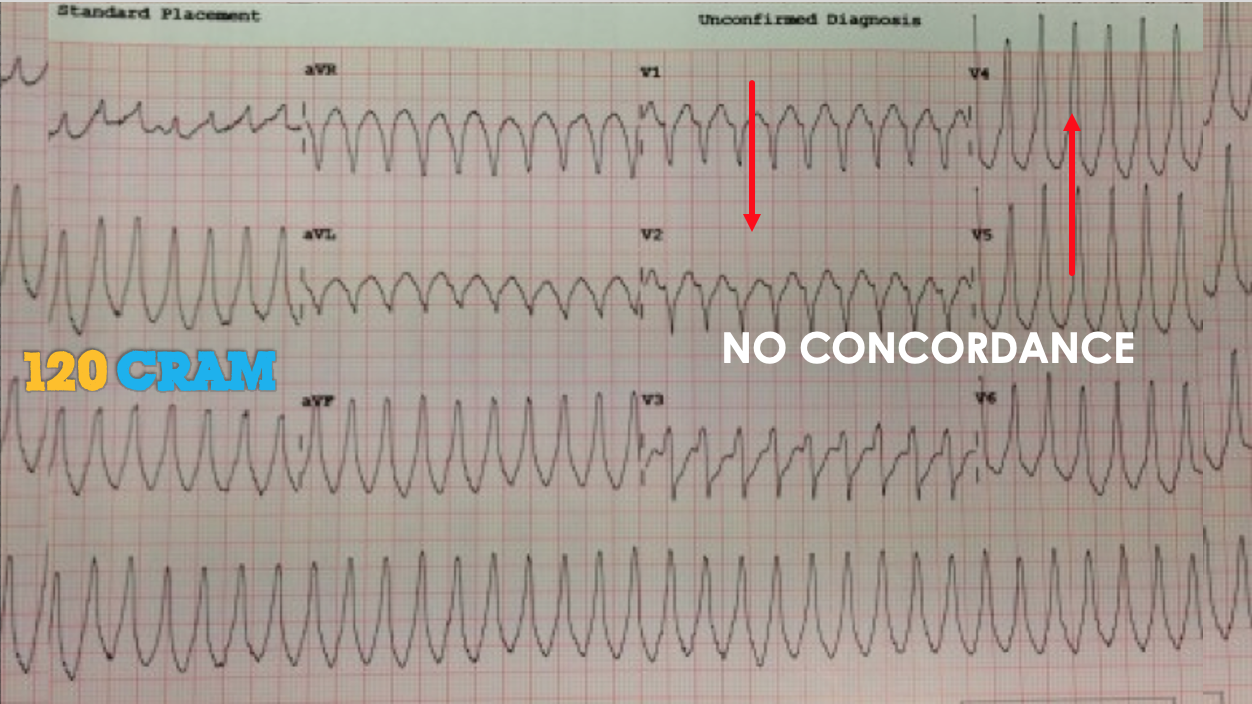 There is no Concordance
There is no Concordance
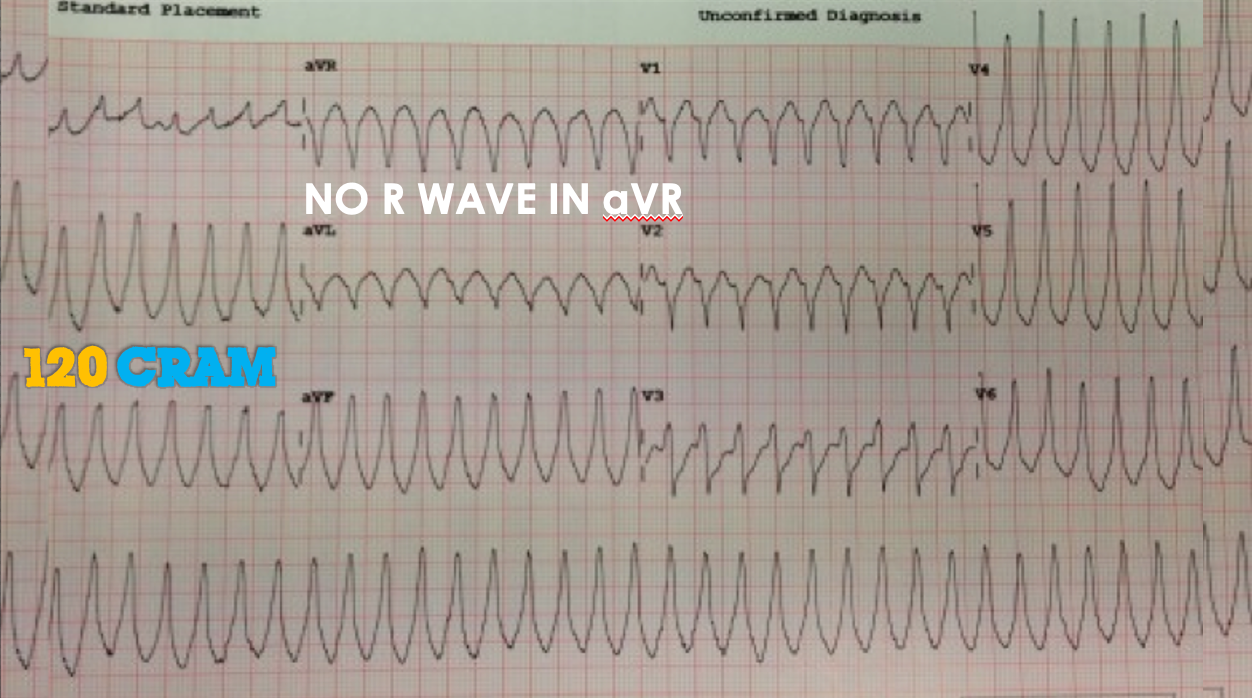 There is no dominant R wave in aVR
There is no dominant R wave in aVR

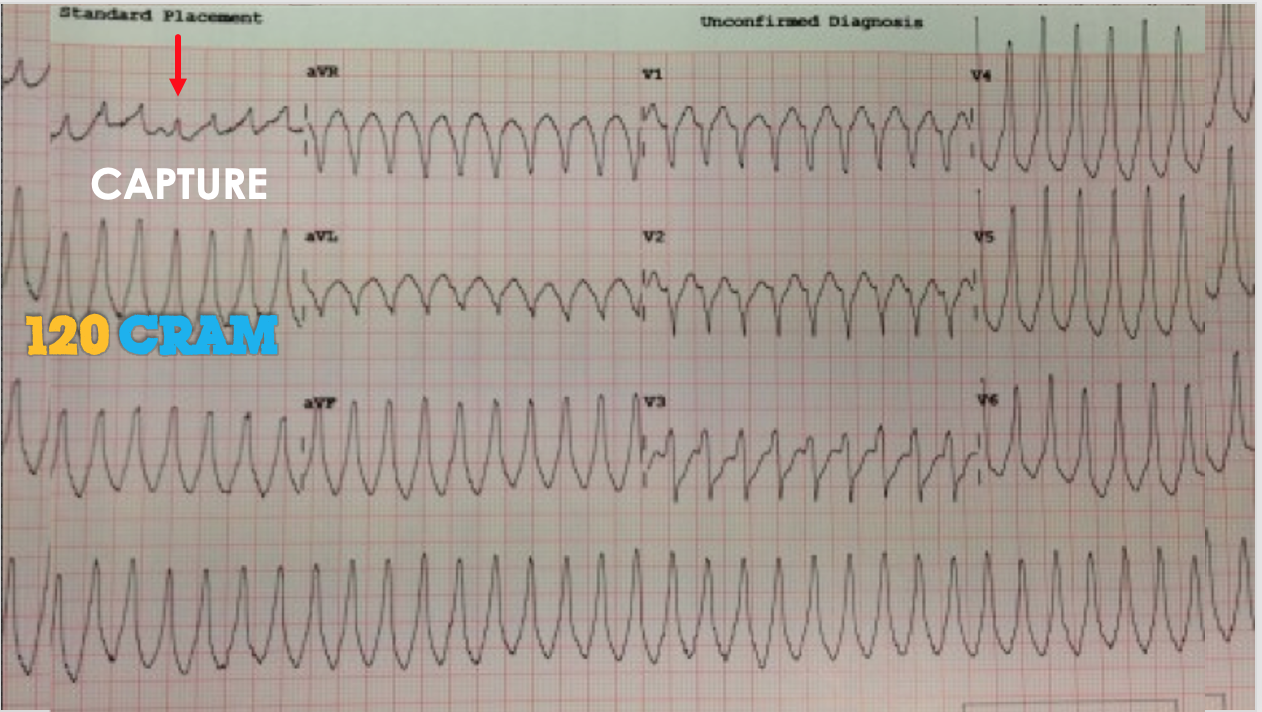
Is this AV dissociation? Probably not. If it were we can call it VT at this point.
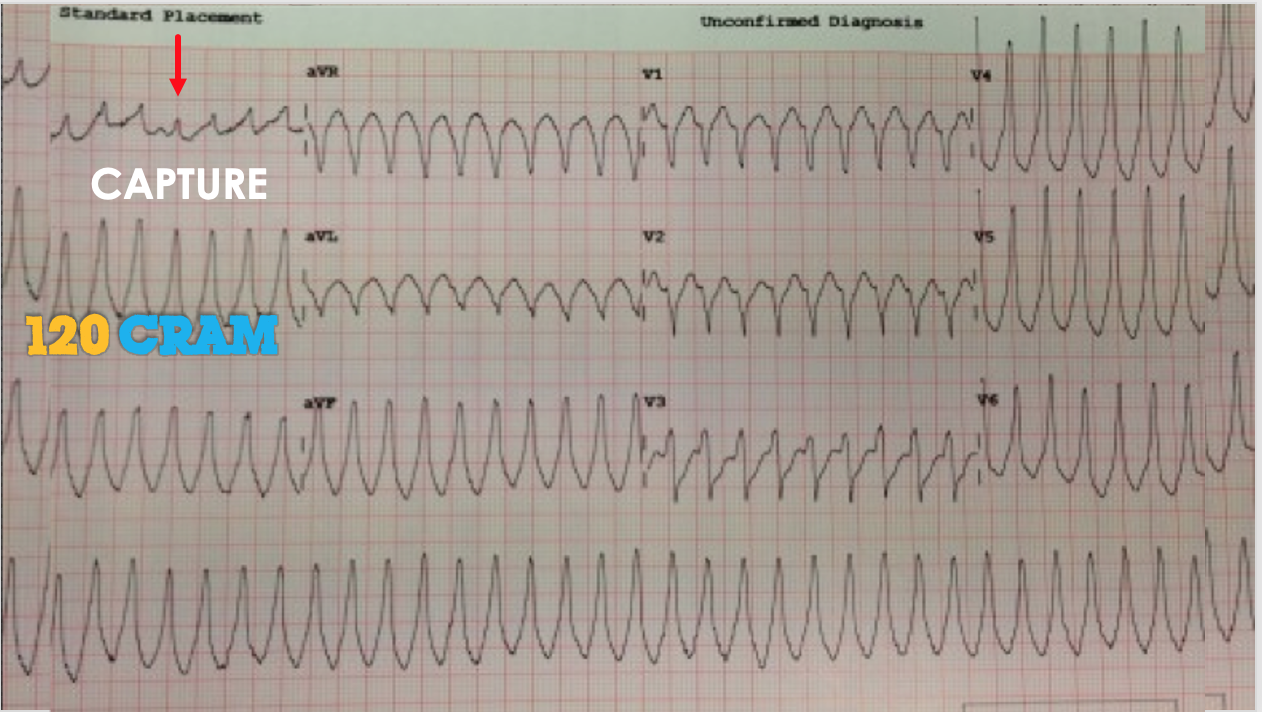
Is this a capture beat? If it is we can stop here. Let’s keep going.
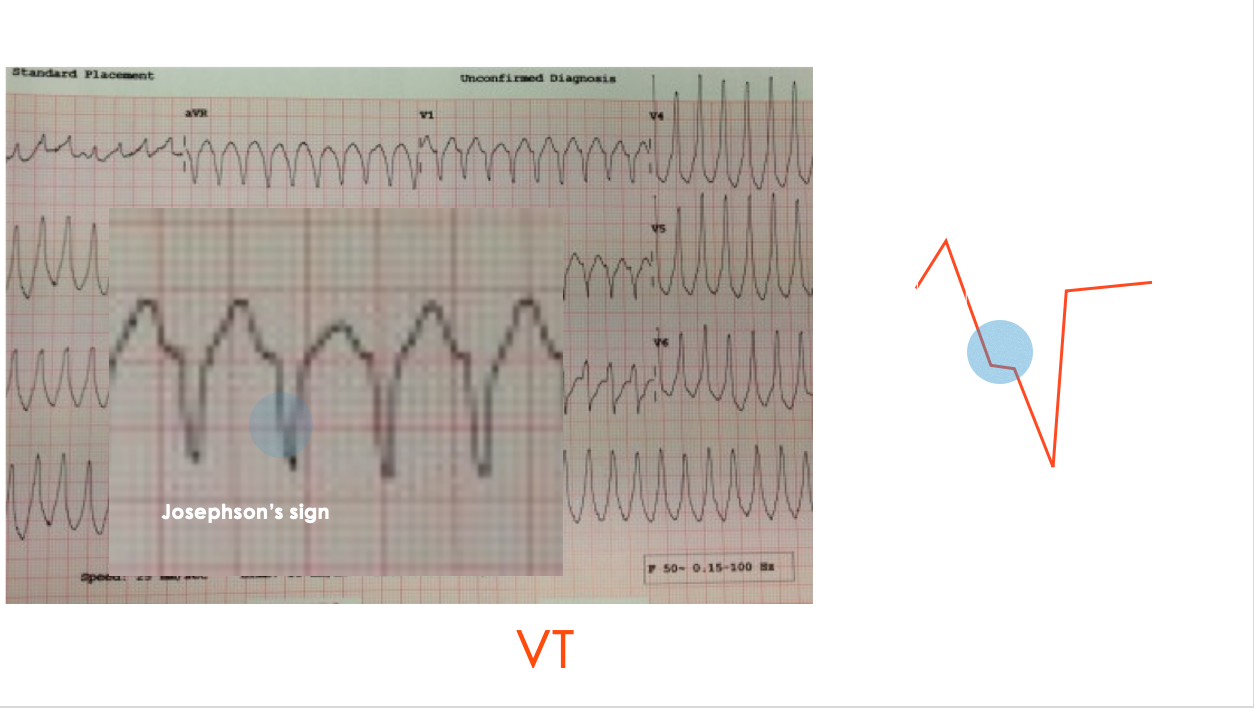 This is LBB morphology, so we look for BRUGADA or JOSEPHSON’S Sign. There is a Josephson sign. THIS IS VT.
This is LBB morphology, so we look for BRUGADA or JOSEPHSON’S Sign. There is a Josephson sign. THIS IS VT.
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Module 4.2 Arrhythmias: Narrow Complex Tachycardias
In this section we look at:
- Wide Complex Tachycardias
- Regular
- Irregular
- Narrow Complex Tachycardias
- Atrial Fibrillation and Flutter
- Blocks
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Module 4.3 Arrhythmias: Atrial Fibrillation
In this section we look at:
- Wide Complex Tachycardias
- Regular
- Irregular
- Narrow Complex Tachycardias
- Atrial Fibrillation and Flutter
- Blocks
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Module 4.4 Arrhythmias: Atrial Flutter
In this section we look at:
- Wide Complex Tachycardias
- Regular
- Irregular
- Narrow Complex Tachycardias
- Atrial Fibrillation and Flutter
- Blocks
This is content for subscribers.
For less than the price of a cup of coffee a week, you can get full access to everything
Module 4.5 Arrhythmias: Bradycardia / Blocks
In this section we look at:
- Wide Complex Tachycardias
- Regular
- Irregular
- Narrow Complex Tachycardias
- Atrial Fibrillation and Flutter
- Blocks