
An 80 yo woman presents to the emergency department with the complaint of feeling her legs give way. There has been no syncope, no injuries and the patient had no other clinical symptoms or signs, just the leg weakness. There was no headache, no palpitations, no chest pain, no shortness of breath, or abdominal pain ( review The SYNCOPE PLUS RULES).
An ECG was done as shown below, with an initial concern of ischaemia.
What does the ECG show?
An ECG was done as shown below, with an initial concern of ischaemia.
What does the ECG show?
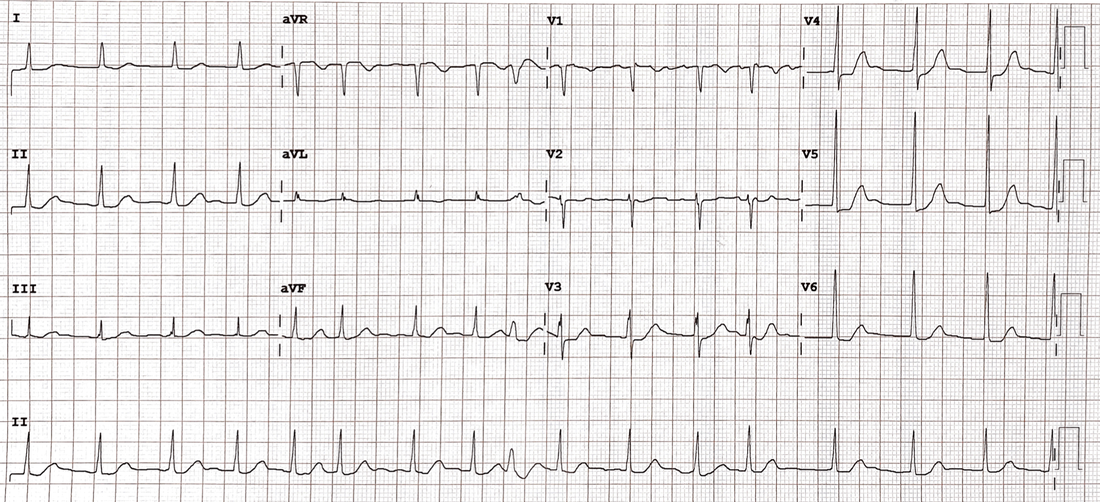
Using the ECG in 20 seconds approach the following are obvious:
- Irregularly irregular ie atrial fibrillation
- ST depression in I, II, aVL, V3-V6
What question do you want to ask next?
- “Are these changes old or new?”
- “Is the patient on digoxin?”
As it turns out the changes are old and the patient is on digoxin.
The changes on this ECG are not of classic morphology, so lets look at it a little more closely.
It’s important to understand the changes caused by digoxin
ACTIONS
Digoxin has a very narrow therapeutic index. It is used frequently and has positive inotropic and negative chronotropic effects. It decreases heart rate due to increased vagal activity, whilst shortening the action potential by increasing intracellular Calcium
ECG CHANGES
|
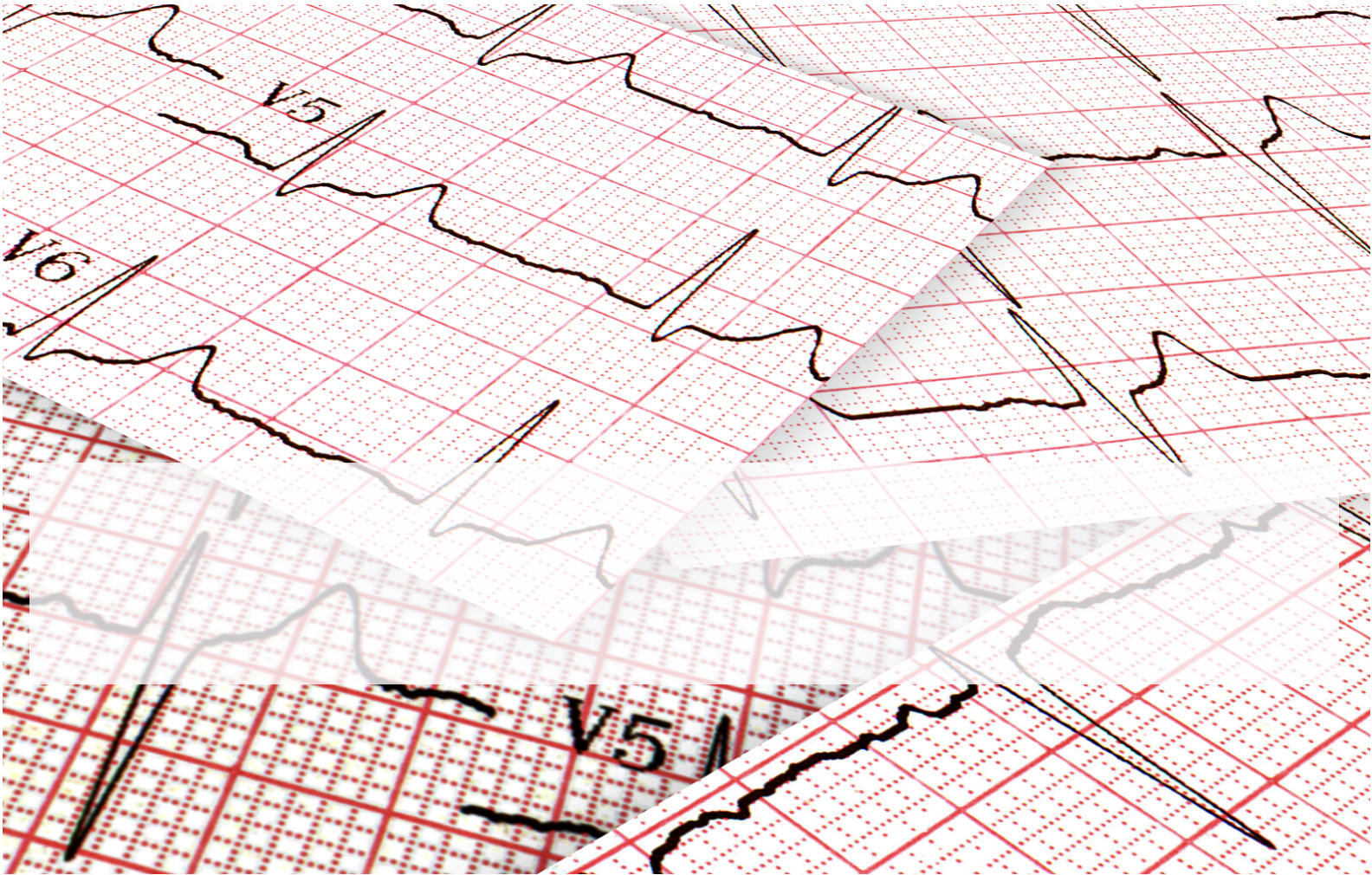
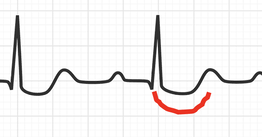
ST CHANGES
There is a downsloping ST depression pattern, in the form of a reverse ‘tick’. This has sometimes been referred to as the Salvador Dali’s(the Spanish surrealist artist) moustache. |
|
|
T WAVE CHANGES
The T wave can be inverted or flattened or biphasic(usually in V4-6). It can look upright in its terminal portion however in most cases this is a U wave.
QT CHANGES
There is usually QT shortening
ECG CHANGES DO NOT EQUAL TOXICITY
It is important to remember that the changes seen on ECG are due to the patient being on digoxin. They do not necessarily indicate toxicity.


