

In preparation for EMCORE Hong Kong 2018, I took some time to sit down and revisit how and why we do one of the oldest rituals in trauma medicine – applying a rigid c-collar. I still remember as a junior doctor being taken through the rigorous method of application….measure up properly, hold the head steady, slide the collar under the nape of the neck and bring it around slowly and carefully to perfectly immobilise the neck. Seriously, there would be bomb technicians trained with less painstaking finesse than I was!
Now, reflecting in 2018, it’s interesting to wonder if we really need to keep going with a hard collar. Some ambulance services (Queensland’s among them) have moved to a soft collar. My take on the theory being it is a reminder to both the patient and care providers to remember not to get all WWF with the neck, whilst simultaneously not going through the rigmarole of a hard collar.
So here’s the real question….was there ever any evidence for a hard collar in the first place? Sure, there’s lots of opinion. Statements like “you simply cannot ignore the anatomy….the spinal cord is at risk when the neck is FLEXED and ROTATED…this must be prevented at all costs!” abound on the internet. But is there actually any evidence?
Now, an important disclaimer – I am writing here and giving my own opinion. I’m not speaking as your supervising consultant or providing practice advice. I am however trying to make you think about why you do your business.
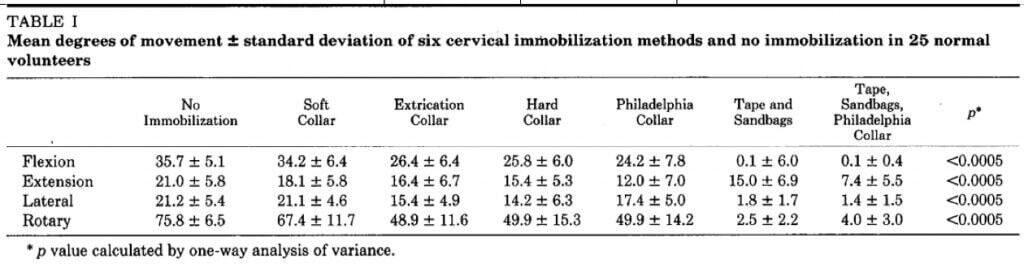
So let’s go back to the key question – is there any reason to use a hard collar? Again my take on the theory is that the aim is to prevent re-movement of the neck, and a subsequent avoidable injury. It’s pretty hard to argue that a hard collar does not minimise neck movement:
Podolsky et al 1983 J Trauma
The genesis of the underlying idea is that secondary injury does exist. As far back as 1988 Toscano described a series of patients taken to hospital with suspected spinal injuries. A number of the patients developed new neurology during the course of their treatment and transfer, and this was attributed to the phenomenon of secondary spinal injury. The broken spine was moved, and so an injury occurred.
Here’s the thing – that’s correlation….not causation. The two are very different. If you don’t believe me, head on over to www.tylervigen.com/spurious-correlations, where you can find graphs like the one below.
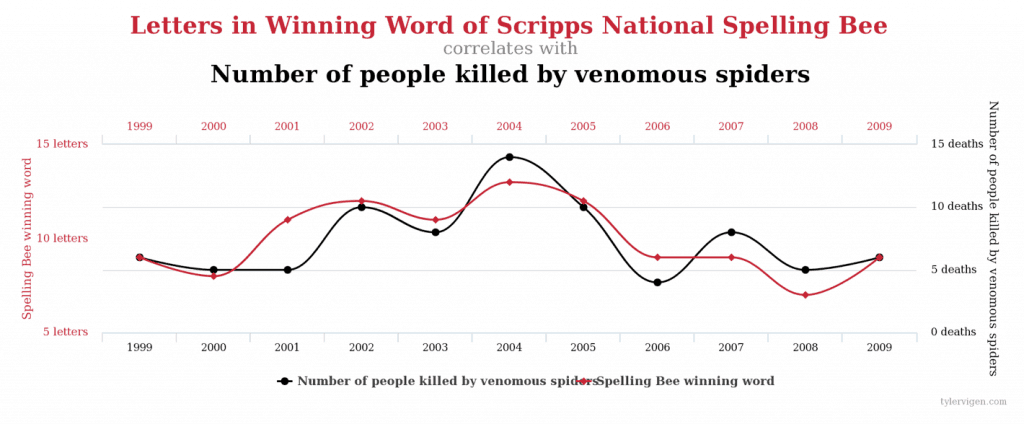
Now, looking at that, you’d swear that when a more difficult word is required to win the US Scripps National Spelling Bee, more venomous spiders kill people. But while there is a clear correlation, there’s not necessarily a reason to believe that one variable affects the other.
What does this have to do with c-spines? Same argument really. Step back for a moment, and have a think about the last time you gave yourself a twisted ankle, or better yet avulsed a malleolus. What did your ankle look like at 2 hours? Swollen? Red? Deformed? It’s the same tissue as a spinal column. In other words, after a serious bony injury, isn’t there the potential for localised swelling and tissue injury to occur as part of the natural pathology of inflammation? And if that occurred in an area of confined space, with fragile tissue, say the cervical spinal canal, wouldn’t that perhaps lead to the development (or evolution) of symptoms anyway??
In other words, a key question I have surrounding the assumptions on the need for immobilisation centres around exactly the underlying reasoning. Is there actually cause to believe that a failure to immobilise a c spine really promotes secondary neurologic injury?
I’ll be speaking on this at EMCORE Hong Kong, and answering some key questions:
- Do hard collars reduce C-Spine movement?
- Does it matter?
- In fact, how hard is it to break a c-spine
- Do hard collars really reduce C-Spine movement?
- Do C-Collars actually cause harm?
As a disclaimer I should warn you all that there are no good answers to these questions, but there’s plenty of evidence to use to inform some debating points. Once we’ve got a feel for the outcome of the debate in Hong Kong, we might stick a bit more up on resus.com.au for those interested.
 Dr Luke Lawton, Director Emergency Services, Townsville Hospital.
Dr Luke Lawton, Director Emergency Services, Townsville Hospital.


