
The CASE
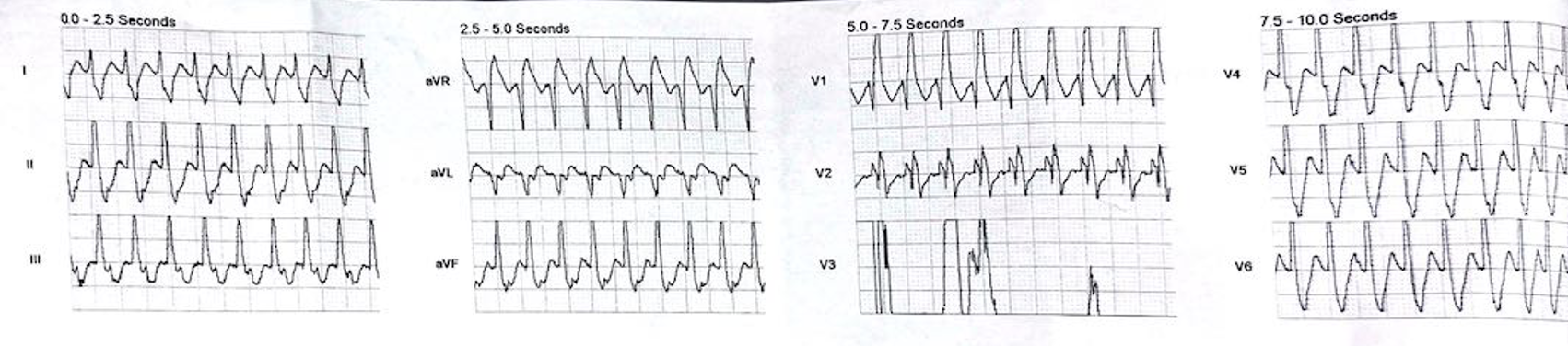
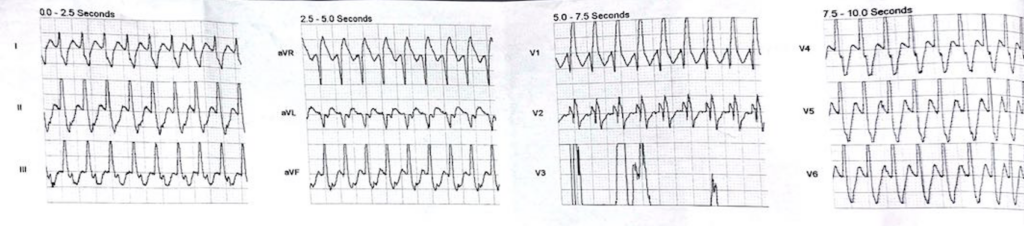
A 45 yo male is brought in by ambulance. They have been called as the patient, who is well otherwise, with no past medical history, has had palpitations. On arrival, the patient is alert, well looking and haemodynamically stable. The following trace is obtained.
Is this VT or SVT with Abberancy or sinus tachycardia with a block?
What would you do for this patient?
The ambulance officers called this a wide complex tachycardia, diagnosed VT and gave Amiodarone. The patient reverted…. I will show you his post reversion ecg below.
A couple of words on haemodynamic status. Patients with SVT, unless they have an underlying cardiomyopathy or other cardiac condition, don’t tend to decompensated and although patients in VT can also have a stable blood pressure, we find that haemodynamically instability is potentially more likely. However this is not a hard and fast rule.
Where they wrong to call this VT?
80% of wide complex tachycardias are VT. As long as it is regular, we can give an AV nodal blocker. Beware the irregular very rapid tachycardia as it may be atrial fibrillation with WPW and an AVN blocker will result in ventricular fibrillation.
If I apply the 120CRAM formula that I tend to use.
- It is faster than 120 bpm and wider than 120 ms so we can proceed to look for VT
- There is no concordance in the precordial leads
- There is a dominant R wave in aVR, so I could have called it VT…….
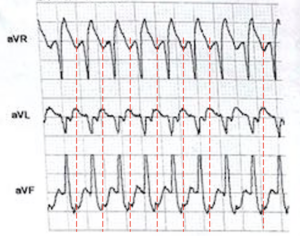
However I can see regular p waves in leads III and aVF. So it is probably SVT with aberrancy.
The patient reverted into a sinus rhythm. The ECG is shown below. What is your diagnosis?
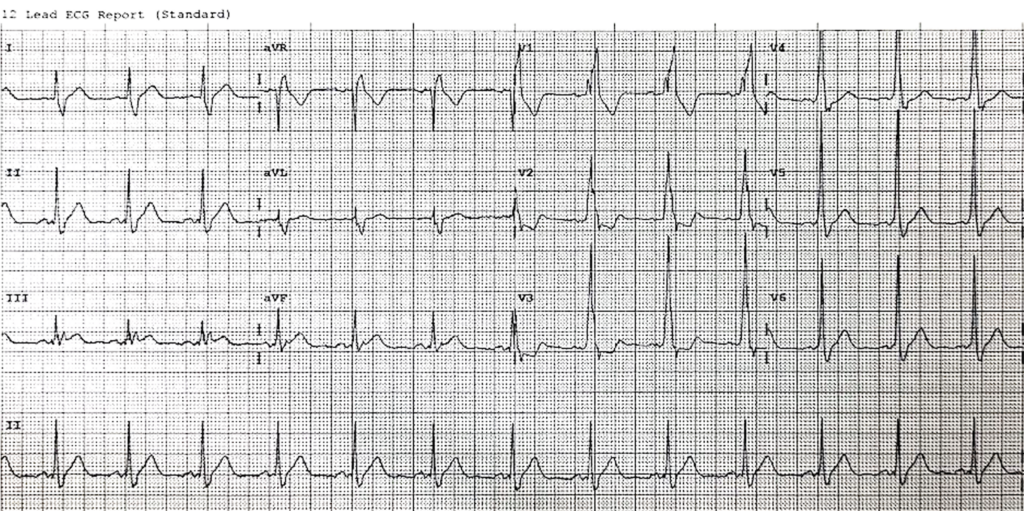
I think that there is a short PR interval here due to a delta wave. So I would call this Wolff-Parkinson-White.
Given that the patient was stable and well. He was commenced on a beta blocker, booked for an outpatient echocardiogram and discharged for outpatient cardiology followup.


