

THE CASE
A 35 year old woman, who is a known intravenous drug user, is admitted with septic shock secondary to bacterial endocarditis. She is acidotic and hypotensive. Her ECG is shown. Here are 2 questions to answer before you look at the answer below.
- Is this an acute Myocardial Infarction(AMI)?
- There is no cath lab in your hospital. Would you thrombolyse if she presented early?
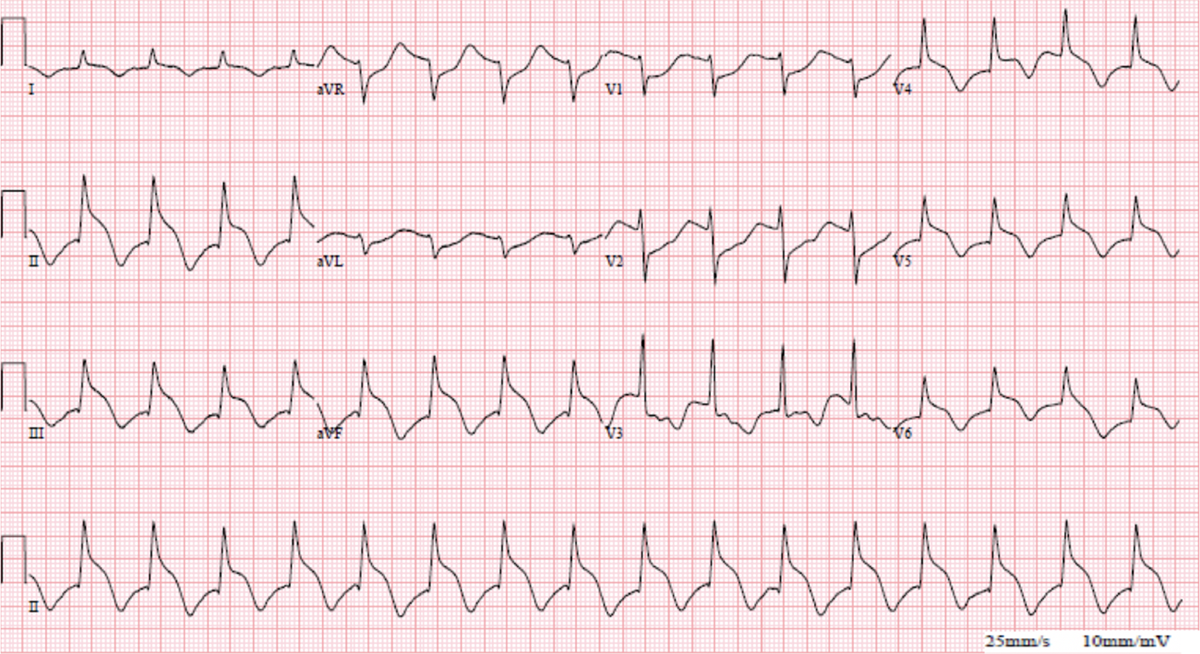
This is an AMI mimic and not a true AMI. The elevation preceding the QRS is not consistent with acute coronary syndrome. The cause of this is thought to be due to a hyperadrenergic state. It is seen in:
- acute abdominal pathology
- intracranial haemorrhage
- sepsis
It’s important to know that this is a pseudo-ST elevation, ie., not an acute myocardial infarction.
The QRS-ST segment resembles a Prussian military helmet and is thus known as the spiked helmet sign.
Reference
- Crinion D et al. An Ominous ECG Sign in Critical Care. Circulation. 2020;141:2106–2109