
The QRS
When it comes to the QRS complex there are 4 questions to ask:
- Is it TALL or SMALL?
- Is it WIDE/NARROW?
- Does it have abnormal MORPHOLOGY i.e. DELTA wave
- Are the complexes CLUMPED or irregularly irregular?
- Are there Q waves?
Is it TALL/SMALL?
If the complexes are TALL– think of left ventricular hypertrophy.
There are several voltage criteria that can be used. I use:
S in V1 + R in V5/6 > 35mm
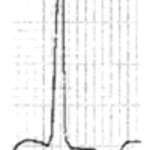
The lateral leads are the best place to view this. There is a large R wave, with a down-sloping ST segment and an asymmetrical inverted T wave.
In situations where the complexes are tall, think about cardiomyopathy, especially Hypertrophic Obstructive Cardiomyopathy.
Some distinct features to look out for include:
- High voltages
- Very thin QRS complexes, especially in the anterior leads
- Q waves in the lateral leads, that are <1mm wide and so do not fit the normal pattern of post infarction Q waves.
If the complexes are SMALL, think of:
- Pericardial Effusion
- Pleural Effusion
- Obesity
- COPD
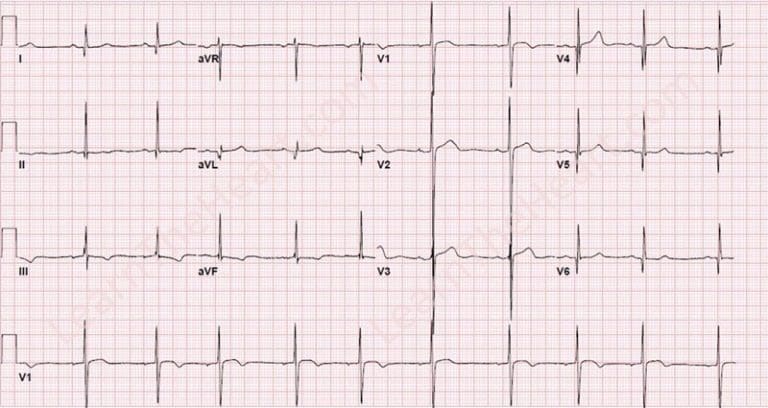
The story may give it away. In a previous fellowship examination, the ecg below was given, with the story of a 63 year old female patient with recent CABG, who now presents short of breath with a tachycardia.
The story may give it away. In a previous fellowship examination, the ecg below was given, with the story of a 63 year old female patient with recent CABG, who now presents short of breath with a tachycardia.
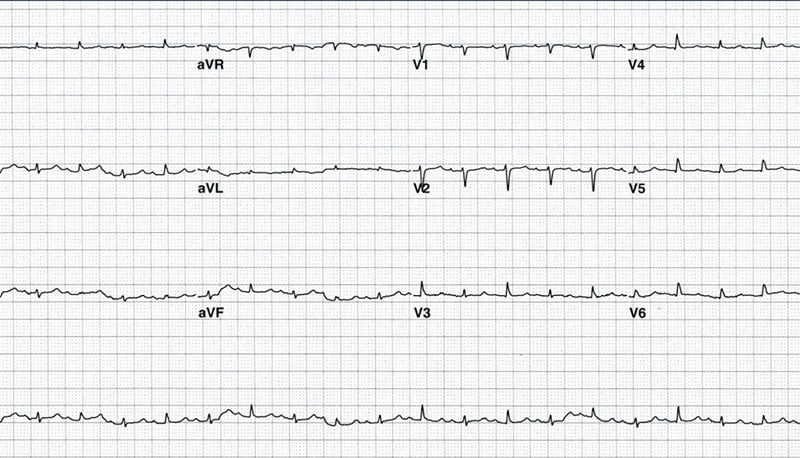
Notice the small complexes. Also notice the electrical alternates, with every alternate QRS complex being of difference amplitude. This is due to a pericardial effusion. The heart swings in an abnormal fashion due to the effusion and the complexes become abnormal.
Is it WIDE/NARROW?
A NARROW complex is defined as < 3 small squares i.e., <0.12ms. This indicates normal conduction through the Atrioventricular node.
A WIDE complex is defined as > 3 small squares.
A wide complex can be:
- a bundle branch block- LBBB or RBBB
- Hyperkalaemia
- Na channel blockade
If the rate is faster than 120 beats per minute think of:
- Ventricular Tachycardia
- SVT with aberrancy
- Antidromic SVT
a side note on axis
One of the few times I calculate axis is with a Right Bundle Branch Block. If this is present then it is important to see if there is a leftward axis. A left axis is caused by a Left Anterior Fascicular Block. If there is a right bundle branch block and a left anterior fascicular block, it means that only the right posterior fascicle is still intact. It may explain the patients syncopal episode. If there is also a first degree block, this is names a triphasicular block and the patient, if symptomatic requires a pacemaker.
The other times that I look at an axis are:
- If I’m looking for an extreme axis in ventricular tachycardia; although this will not usually make the diagnosis./li>
- If I’m looking for a right axis in a potential pulmonary embolism
Back to WIDE Complex
To diagnose VENTRICULAR TACHYCARDIA, I look for the following:
- Is the patient presenting with the right history for this? i.e., are they older, with risk factors, or know heart disease?
- The rate must be > 120 beats per minute
- Beware: If there is a wide complex tachycardia, but the rate is not > 120, it may not be ventricular tachycardia. Think of:
- Hyperkalaemia
- Na channel blockade
- Beware: If there is a wide complex tachycardia, but the rate is not > 120, it may not be ventricular tachycardia. Think of:
- The complex must be wide- wider the better but > 3 small squares
- Is there concordance?- Are the complexes in anterior leads pointing in the same direction?
- Is there AV dissociation? Can you see P waves?
- Are there Fusion Beats?
- Are there Capture Beats?
- Is there an Rr complex in V1? Is there a rabbit ear in V1?
- Is there a Josephson’s Sign?
- Is there a Brugada Sign?
- Is the Axis Extreme?
Are the QRS’s clumped?
This is a reminder to look for the MOBITZ block. If the QRS complexes are clumped, usually regularly, unless you have a variable block or atrial fibrillation, then think of a MOBITZ Block.
Are there Q waves?
If there are Q waves, look for two things:
- Are the Q waves long and thin i.e. < 1mm, think Hypetrophic Cardiomyopathy
- If they are > 1mm, the patient may have had a previous infarction.


