
The ST-T Segment
The first point to make is that the baseline to use when reading the ECG is the T-P Line. This allows you to quickly pick up ST depressions and elevations.
The ST changes that can occur, can be ischaemic and in some cases due to arrhythmias.
ST Elevation
It is imperative to differentiate between ST elevation of acute myocardial infarction vs Early depolarisation, vs acute pericarditis.
Causes of ST Elevation:
- Acute MI
- Benign Early Repolarisation
- Pericarditis
- LV Aneurysm
- Vasospasm
- Bundle Branch Block
Morphology of STE
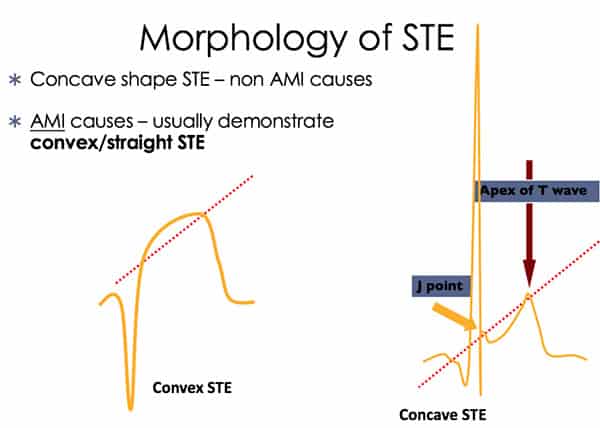
Look for STEMI in all the arterial territories: Inferior, lateral and anterior. Also keep in mind the posterior MI and the potential for a right ventricular MI in inferior infarction.
Subtle ST Signs of MI
Sometimes the signs of an MI can be very subtle. There may be no more than a peaked T wave. Or a QRT sign, where the T wave comes directly of the R wave.
There may be reciprocal changes, but they are not always there.
Benign Early Repolarisation
- STE <2 mm
- Concavity of initial portion of the ST segment
- Notching or slurring of the terminal QRS complex
- Symmetrical, concordant T wave of large amplitude
- Widespread or diffuse distribution of STE
- Does not demonstrate territorial distribution
- Relative temporal stability
Acute Pericarditis
Stages of Pericarditis: These may not always be present.
Stage 1
Concave ST elevation in praecordial leads V5,6 and I
PR depression II, aVF, V45
Stage 2
ST segments normalise to baseline
Decreased amplitude in T wave
Stage 3
T inversion – days to weeks
Stage 4
Resolution to normal
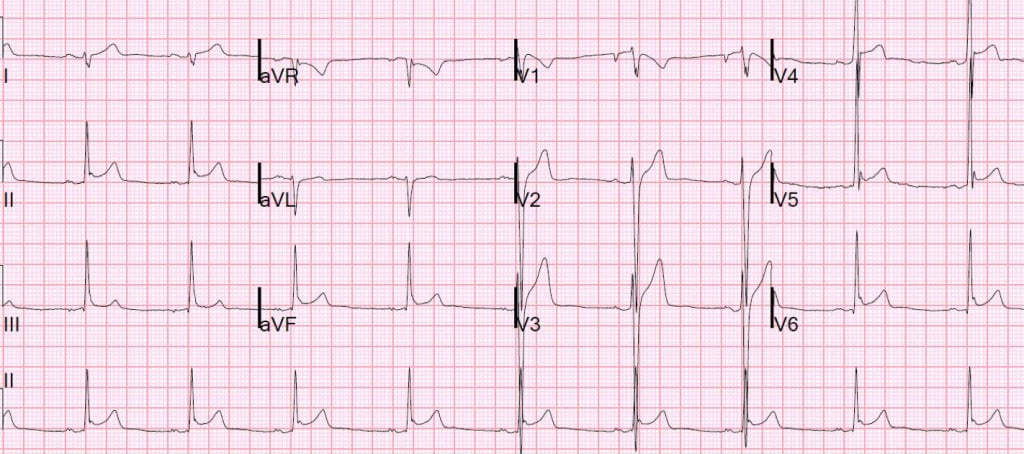
Beware of avR
St elevation in patient with ischaemic symptoms can be indicative of AMI. There is usually an ST elevation in avR with widespread ST depression in other leads. Usually there should > 5 other leads with ST depression.
It does not apply to asymptomatic patients.
- ST elevation in aVR >1.5mm = 75% mortality
In this subgroup, thrombolytics don’t work, they need cath and potentially CABG
- ST elevation in aVR + aVL >95% specific for LMCA
- aVR>V1 = prox LAD or LMCA occlusion
Other Causes of ST Elevation
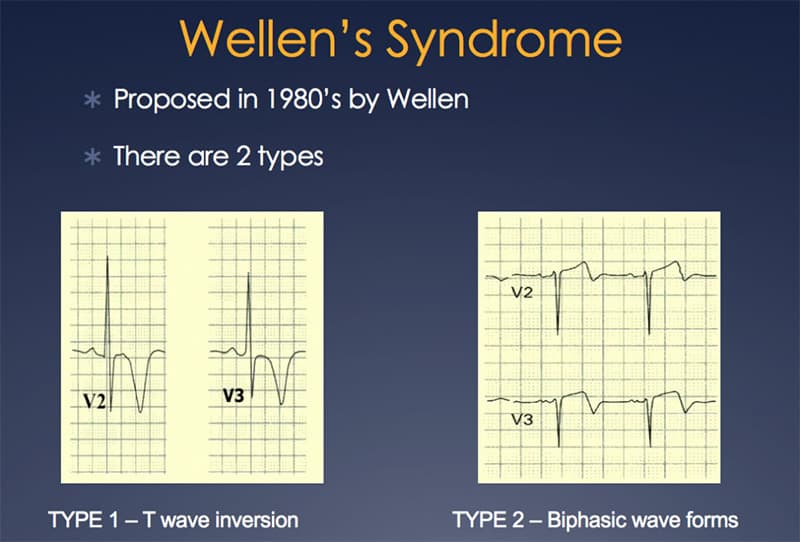
Wellens Syndrome
Wellens patterns tend to occur on the ECG, when the patient is pain free and there may be no troponin sire. It does however represent LMCA occlusion. No thrombolysis should be given unless ST elevation.
Beware pseudo-wellens. Wellness cannot be diagnosed in the presence of left ventricular hypertrophy
Other Causes of ST Elevation Patterns
Beware Brugada Syndrome. This is a Na channel abnormality that results in a tornadoes-type rhythm. If it self terminates, the patient will present with syncope, if it doesn’t, they present in cardiac arrest.
There are two main patterns: coved or saddle-shaped


