
A 74 year old man who has presented with seizure-like activity. He was not post ictal. Following this he had a cardiac arrest that was death with, with CPR and he quickly regained return of spontaneous circulation. He is now speaking and awake. His ECG is normal sinus rhythm, but you notice his rhythm strip when he first presented. It is a wide complex tachycardia presumed to be Ventricular Tachycardia, that has lasted for approximately 20 seconds. He has had no further episodes. Your working diagnosis is that the Ventricular Arrhythmia has caused the seizure-like activity.
According to my 3 rules for diagnosis VT, if all 3 are positive treat as VT:
- The QRS is wider than 120ms
- The rate is faster than 120
- It is real, ie., not artifact.
This therefore VT.
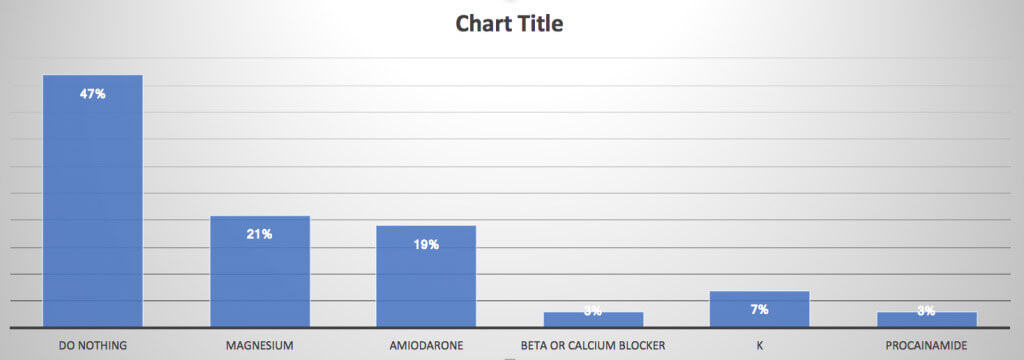
The question I ask is, what do we do? The options are:
- Do nothing
- Give Mg 10mmol/L
- Give Amiodarone
- Give Metoprolol or Ca channel blocker
- Give Potassium
- Give Procainamide
The recent survey results were very interesting. Approximately half of the group would do nothing in terms of treatment and about one fifth would give magnesium and one fifth would give amiodarone.
The literature is not clear cut on all of this, however clear enough that we know what to do.
In all cases we should ensure that electrolytes are normal. Therefore by all means top up the potassium and top up the Magnesium Sulphate. Here is an overview of both non-sustained and sustained VT.
NON-SUSTAINED VT(NSVT)
The definition of non-sustained VT varies in the literature. The rate varies from greater than 100 to greater than 120 beats per minute, the duration of the beats varies and even the total number of beats varies.
We don’t know the significance of NSVT in healthy individuals. In athletes they have no adverse prognosis. In non-athletes, they may represent a greater risk of death if they occur during exercise recovery, rather than during exercise.
The underlying heart conditions we must look for include:
- Coronary Artery Disease
- Cardiomyopathy
- Hypertension
- Channelopathies
- Valve Disease
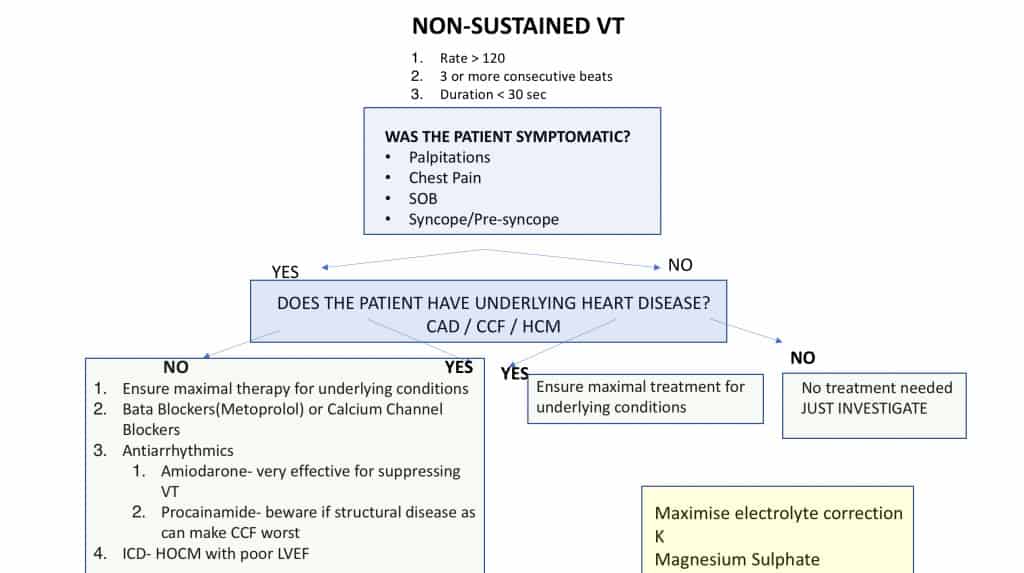
An Approach To NSVT
Was this NSVT?
The definition we will use is a widely accepted one:
- Rate >120
- 3 or more consecutive beats
- Duration is < 30 seconds
Was the patient symptomatic?
Symptoms can include chest pain, palpitations, dyspnoea and syncope, or altered conscious state.
Does The Patient Have Underlying Heart Disease?
This may sometimes be difficult to know. It usually refers to a reduced Left Ventricular Ejection Fraction or Cardiac Failure.
If there are no symptoms and no heart disease, then no treatment is needed.
If the patient has no symptoms but does have underlying heart disease, and the NSVT is an incidental finding, ensure their treatment for their condition is appropriate and maximised.
- If the patient does have symptoms, ensure their medications are appropriate if they have heart disease and treat them whether heart disease or not with appropriate medication:
- This is usually Beta blockers or Ca channel blockers, in more of an outpatient setting
- Antiarrhythmics are used in the Emergency Department
- Amiodarone is very effective in suppressing VT
- It can be used in patients with underlying heart disease.
Below is the approach to the patient with NSVT
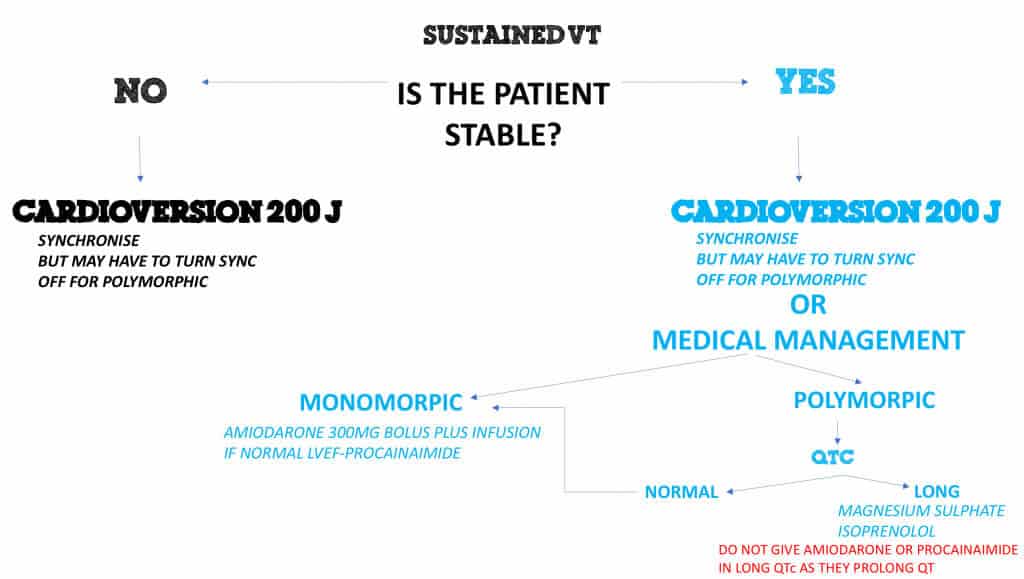
SUSTAINED VT
An Approach To The UNSTABLE Patient.
If the patient is unstable, which is judged by end organ involvement ie, chest pain, dyspnoea, haemodynamic compromise, then CARDIOVERSION can be used. Use 200J. Beware in polymorphic VT, as the defibrillator may have trouble picking up the R wave. In this case, turn sync off.
An Approach to the STABLE Patient
If the patient is stable CARDIOVERSION can still be used. If alternative medical treatment is considered, then its is a matter of what type of tachycardia it is.
Monomorphic Tachycardia.
If there is a normal Left Ventricular Ejection Fraction(LVEF), then Procainamide or Sotalol can be used
If there is an abnormal LVEF then Amiodarone should be used as Procainamide may exacerbate heart failure.
Polymorphic Tachycardia
Polymorphic tachycardia, normally self terminates, however it recurs. During one of the reversions to sinus rhythms and ECG must be done and the QTcorrected interval must be calculated.
If the QTcorrected is normal treat as for monomorphic VT
If the QTcorrected is prolonged, treat with Magnesium Sulphate and Isoprenelol.
BEWARE: Amiodarone and Procainamide are contraindicated in PROLONGED QTc, as they can further prolong the QT interval.
Below is the Approach to the Patient with Sustained VT
Conclusion
In our case study we had a patient with non-sustained ventricular tachycardia, who was symptomatic. The symptoms were the seizure-like activity, with no-post ictal component, Therefore, the seizure activity probably represented a response to the patient dropping their blood pressure. We have no idea of underlying heart disease in this case when the patient presented. The options in this patient were to start a beta blocker, however in the acute setting, Amiodarone is the appropriate drug to start.


