
A Case of Severe Metformin Toxicity
The call comes in just after midnight. A 67 year old male has been brought to the Emergency Department. He had complained of lower back pain, feeling unwell, with two episodes of vomiting.
He arrived in the Emergency Department, aggitated, complaining of severe pain and having already been given, 370mcg of Fentanyl by the ambulance. His past history is of Hypertension and Diabetes and he takes Amlodipine and Metformin.
His vitals were: T 30.9, HR 60, Resp Rate 36, BP 100/35, GCS E1,V2,M4 =7
The initial venous gas is shown below:
FiO2 0.8
pH 6.74
pCO2 20
pO2 110
O2 sat 89%
BE <-30
HCO3 3
Lactate 19
 A rapid clinical examination demonstrated, clear lungs, a soft abdomen and a FAST scan of the abdomen was normal.
A rapid clinical examination demonstrated, clear lungs, a soft abdomen and a FAST scan of the abdomen was normal.
The patient was intubated using Ketamine and Rocuronium and a size 7.5 endotracheal tube was passed. The airway was a Cormach Lehane grade 4.
100mmol of NaHCO3 was given intravenously to treat the low pH.
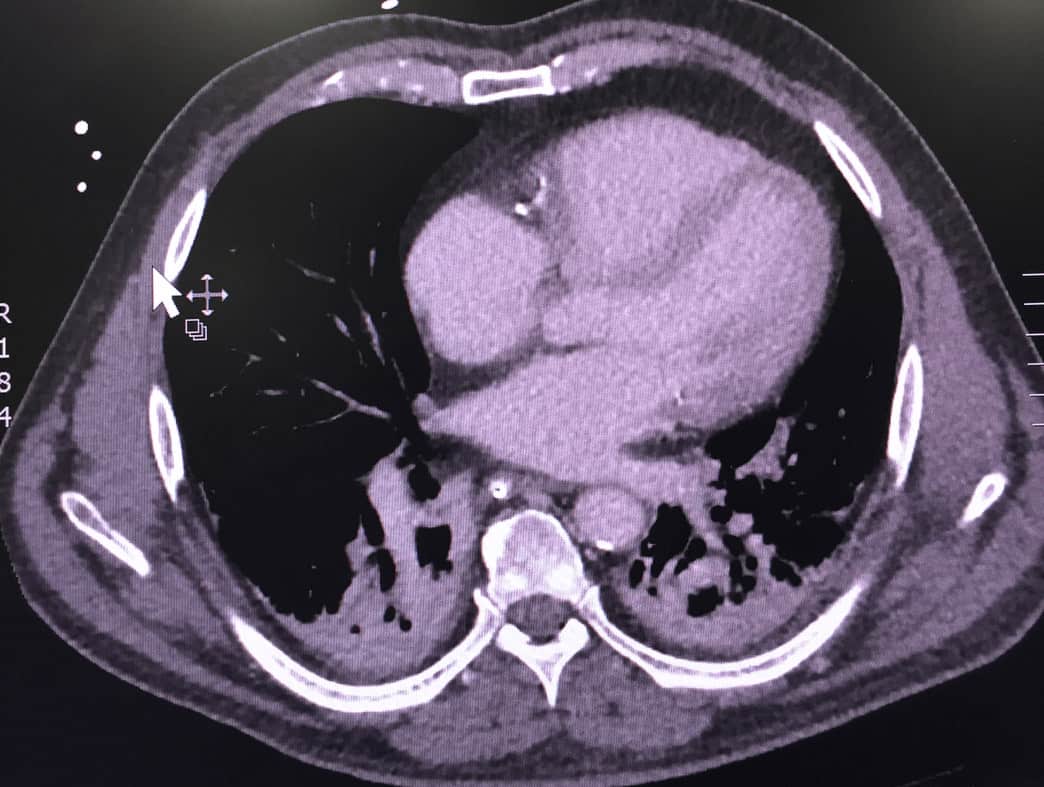
A CT scan of the chest and abdomen was performed, looking for a cause for the patient’s back pain and high lactate ie., was there an ischaemic bowel, or a large aorta. The findings were some dependent atelectasis in the lungs and one atrophic kidney.


Due to the atelectasis on CT, Ceftriaxone was given initially with an antivirals. Pip-tazidine was added iven that sepsis was the concern in this patient (even though he was not febrile) pip-tazidine was added.
The patient’s Blood Pressure became somewhat volatile via a Non- Invasive Cuff and so an arterial line was inserted, reading a systolic BP of 80mmHg.
Peripheral Metaraminol was used in 1mg boluses, to maintain blood pressure and a Metaraminol infusion was commenced.
A further set of gases was taken without much improvement in acidosis.
A central line was placed.
During this time the patient’s blood pressure continued to drop. A noradrenaline infusion was commenced. With very little improvement in blood pressure and following a cardiac echo at the bedside, that showed no focal abnormality, adrenaline was commenced.
The patient’s blood results then returned:
Na 139
K 5.3
Cl 96
HCO3 <5
AG >43
Glc 6.7
Urea 27.9
Creatinine 1000
eGFR 4
Hb 118
WCC 24.9 (Neut 18.4)
Plt 292
With the patients Creatinine level and level of acidosis, it was decided that we would dialyse the patient. A Vas catheter was inserted and the patient prepared for dialysis.
The patient went to ICU where Vasopressin was also added to support the blood pressure.
Over the next 24 hours, the acidosis improved. In the following 24 hours the inotropes were decreased and then ceased and the patient awoke and obeyed commands.
By day 3 he was extubated.
WHAT WAS THE CAUSE?
This is a case of severe Metformin Toxicity.
Metformin is a biguanide that inhibits gluconeogenesis and increases tissue sensitivity to insulin. It is minimally metabolised and almost completely excreted by the kidneys.At therapeutic doses and even massive overdoses, it doesn’t tend to cause hypoglycaemia.
Because it blocks oxidative pathways, it results in increased anaerobic metabolism and can cause life threatening lactic acidosis.
How do Patient’s Present?
As lactic acidosis increases, patients will present with nausea and lethargy. The patient will progress to an altered conscious state, tachypnoea and cardiovascular collapse.
Acute Management
The sickest of patients, of which our patient was certainly one, will present with a severe lactic acidosis, with lactate levels > 10mmol/L and will usually have a very high creatinine.
Thos patients with a lactate > 10mmol/L and impaired renal function require dialysis to remove the acidosis and the metformin.
It is appropriate to use NaHCO3, to assist with acidosis in the initial stabilisation. This may also help with the cardiac dysfunction that occurs with acidosis leading to hypotension.
This patient was initially commenced on noradrenaline, following central line insertion. The working diagnosis initially, was sepsis, given the CT report and the high white cell count. We had been running metaraminol prior to this. As the blood pressure continued to decrease, an Adrenaline infusion was also commenced. When in ICU, Vasopressin was also used.
The Result?
The vasopressors kept the blood pressure up whilst the dialysis worked. By day 3, the pH was normal, the patient was producing urine and was extubated.
References
- Bailey CJ.Turner RC. Metformin. NEJM 1996;334:574-579
- Arroyo D et al. Metformin-Associated Acute Kidney Injury and Lactic Acidosis. Int J of Neph. oi:10.4061/2011/749653.
- Price, G. Metformin Lactic Acidosis , Acute renal failure and Refocoxib. Br J Anaesthesia 2003;91:909-10
- Vecchio S, Protti A. Metformin-Induced Lactic Acidosis:No One Left Behind. Crit Care 2011, 15:107


