In this blog we again look at why serial ECGs are important and how to approach a particular ECG variant, where there may be some ST elevation, but not in contiguous leads. We introduce The South African Flag Sign.
CASE
A 54 yo male presents with left sided chest pain that radiates into his jaw. He has vomited once.
His past medical history includes:
- Diabetes
- Hypercholesterolaemia
- An AMI 10 years ago
- Hypertension
This is a great case presented recently at EMCORE by Prof Louise Cullen who has allowed me to use her slides here.
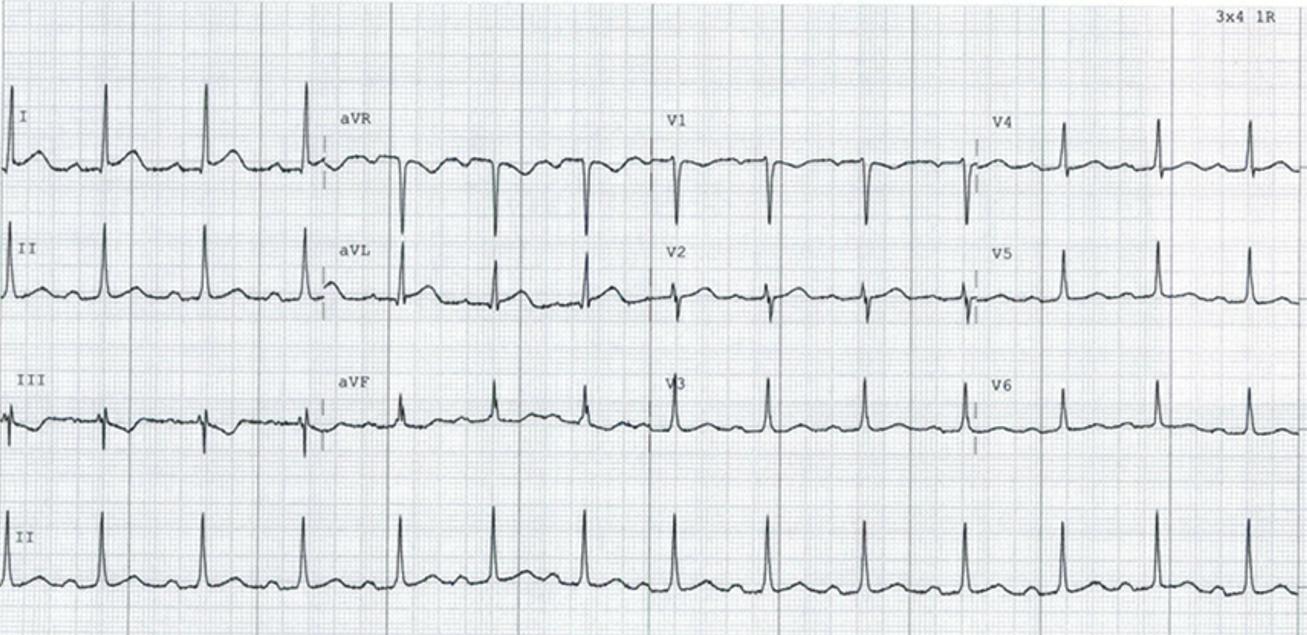
His first ECG is shown below. Describe and interpret the ECG.
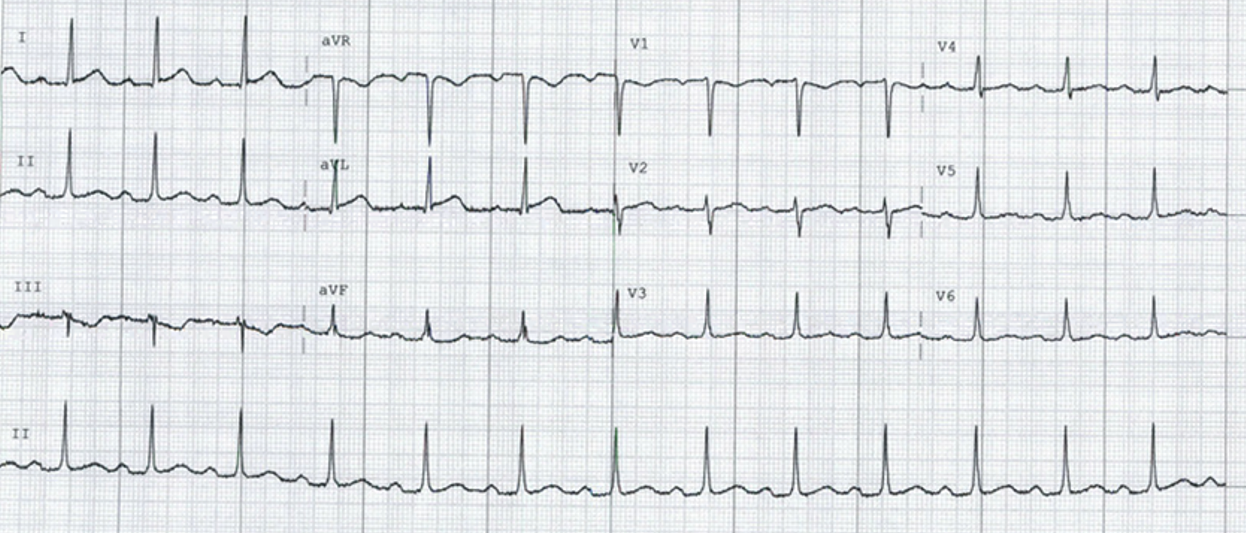
Sinus rhythm
Rate 78
Axis: Normal
Narrow complex QRS
ST segments:
- ? ST elevation I and aVL
- T wave inversion lead III
Intervals: Borderline prolonged PR
Anything else?
Let me ask you this question: Is this a fast rule out candidate? Can we apply ADAPT criteria for rapid rule out? We will need two high sensitivity troponins 2 hours apart and then apply the TIMI Score.
I can tell you that once he has all these risk factors and has had a previous AMI, he is being referred! This is not a rapid rule out patient.
|
|
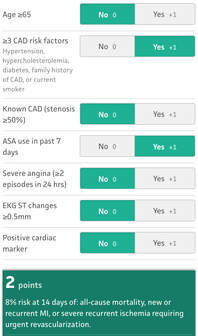
TIMI ScoreThe Thrombolysis in Myocardial Infarction Score looks at the likelihood of ischaemic events or mortality in patients with unstable angina or a NSTEMI. Without knowing a first troponin- the patient has a TIMI score of 2- He is not for rapid rule-out. He is getting admitted. Let’s look at the case in more detail however and see how it unfolds. |
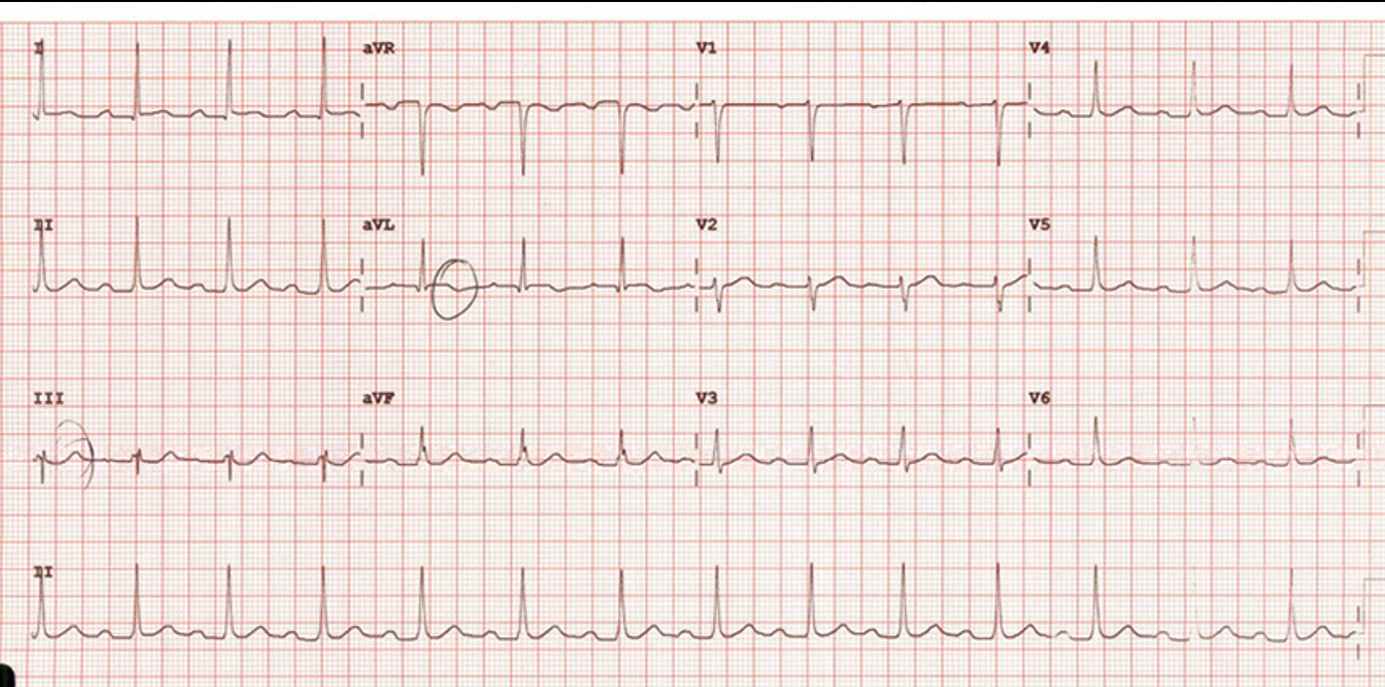
Not much has changed here. Perhaps there is more ST elevation in lead I and certainly aVL. T waves are still inverted in lead III, perhaps some ST depression in III.
The patient has a serial troponin and at 3 hours the troponin is raised, (30ng/L normal is < 20ng/L)
A further ECG is done at 6 hours: Describe and interpret.
A further ECG is done and shown below. The Troponin is now raised at 472ng/L.
How is this ECG different?
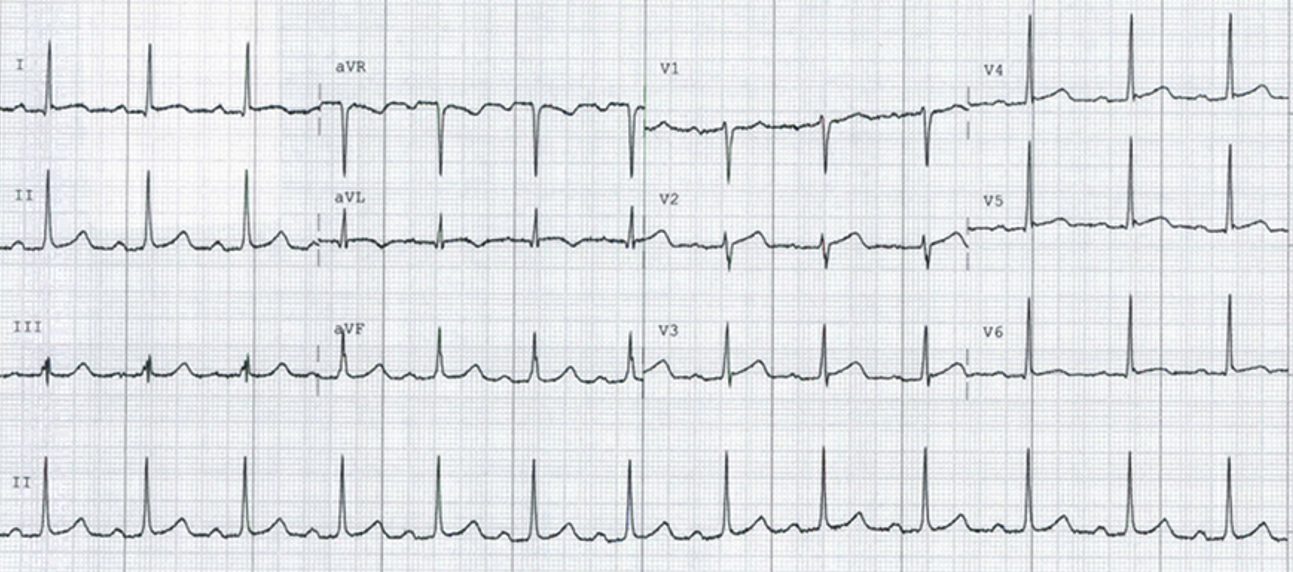
Perhaps we can now see some ST elevation in I and aVL and even in V2. Perhaps the ST depression in III is a little reduced.
The TIMI Score has now increased to 4 and predicts about a 20% chance of MI or ischaemia or all-cause mortality.
The patient was taken to the cath lab and an occluded Diagonal artery was found, for which he had successful PCI.
So the question here is is, without the 6 hour troponin and the fact that there is no ST elevation in contiguous leads, this might be one of those ECG we miss. We need to look at this particular pattern in the ECG.
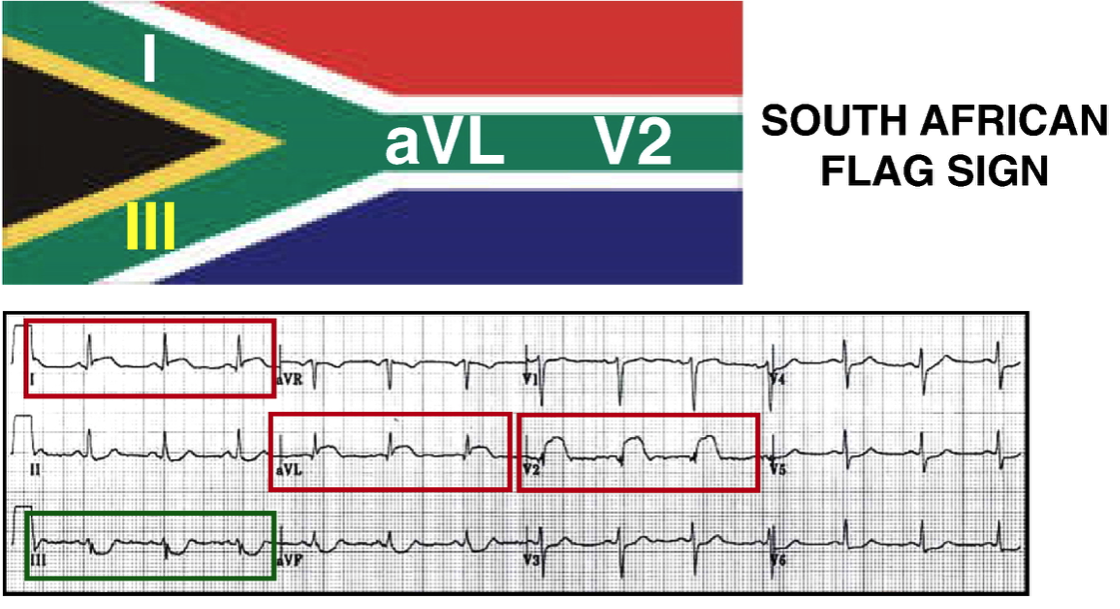
We clearly see the ST elevation in I, aVL and V2 and ST depression in II, III and aVF.
Littman in response to this, discussed the South African Flag sign as a way of memorizing the changes in a high lateral infarct..
The ECG changes were:
- ST Elevation in I, aVL and V2 and
- ST Depression in lead III