

Hi Everyone
I hope you’re holding up out there. As we prepare for the onslaught that may come our way, I’ve been looking at the safest systems we have that we can use. How can we make these as safe as possible, because we don’t have negative pressure rooms in a lot of smaller centres.
We almost take it for granted that Hudson Masks and non-rebreathers are safe, with minimal aerosol spread. I had some doubts and so looked at some of the limited evidence out there.
Before we go to a summary of three oxygen delivery techniques (nasal canal, Hudson and Non-rebreather Masks) here are some general rules I have:
- Use the technique that gives the greatest benefit to the patient, but only if it also gives the greatest protection to the healthcare worker
- The higher the flow, the greater the risk of aerosol production and thus the greatest risk of healthcare worker infection
- Have defined goals of oxygen therapy
- Use minimum FiO2 to achieve goal saturations
- Aim for maximal saturations of 96%
- Most recommendations are for saturations of 90-92%
- I would be happy to achieve 88-92%, whilst minimising aerosol contamination
- No nebulised medications, it’s now all about spacers
- Where possible consider a ‘belt and braces’ approach. Use a surgical mask over nasal prongs, or over an oxygen mask to minimise leakage of aerosols, being careful not to distort the mask.
APPROACH TO THE HYPOXIC PATIENT
Nasal Cannula, Hudson mask and non-rebreather masks are accepted as being Non- Aerosol Generating delivery systems.
Nasal Cannula
We start with nasal canal. Start at 0.5 L/min and go up to 3-4L/min, if the patient can tolerate. This is a relatively safe approach, as long as the patient doesn’t cough. Therefore put a surgical mask over the patient and the cannula. Hui DCS et al found in a simulated manikin study that dispersion distance was at most 0.42m. However we need to be careful here, as this was a simulation and the lung injury simulated was mild. With greater injury comes a potentially larger problem. The ‘smoke’ used to simulate particles in this study may not effectively reflect the behaviour of droplets of various sizes.

Oxygen Mask
 Non-Rebreather Mask
Non-Rebreather Mask
If we need more we usually would progress to a Hudson Mask at 4-8L/min and then to a Non-Rebreather mask at 10-15L/min. HUi’s study demonstrated that the spread of ‘smoke’ from the simulator was less than 0.4m for a Hudson mask and even less ie <0.1m from the non-rebreather mask; which intuitively doesn’t make as sense to me. Why would a non-rebreather at a much higher flow have less spread?
Let’s look at masks a little closer. All the oxygen masks that we use are vented- those little holes with a valve-like mechanism, which aims to minimise entrapment of room air, whilst allow flow out of the mask. In my mind, this is a constant source of expiratory droplets at high flow. Is that right?
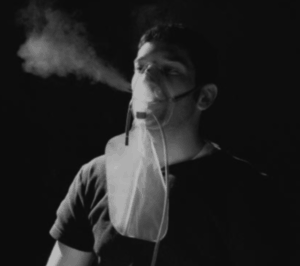
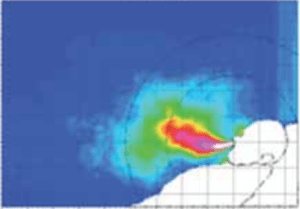
Somogyi et al looked the effects of vent systems in these masks. The subject inhaled aerosolized 3% saline fluid droplets that were produced by an ultrasonic nebulizer, then after holding their breath for 2 seconds exhaled (with no oxygen delivery to the mask). Various oxygen mask types were tested. They were well fitted to the face.
 Comparison was made with the above open vented system, with a system of no vents in the mask and a fitted one way valve and viral filter. It was obvious here that there was a minimal amount of aerosolised saline escaping, when there were no vents in the mask.
Comparison was made with the above open vented system, with a system of no vents in the mask and a fitted one way valve and viral filter. It was obvious here that there was a minimal amount of aerosolised saline escaping, when there were no vents in the mask.
What does all of this mean?
- Try to fit a surgical mask over all of these systems
- Care for the patient in such a way that you maintain a distance of a minimum of 0.5 1.0 m from the face. This may not always be possible.
- In a study comparing HFNC and oxygen masks, Leung found that bacteria(looked at pneumonia patients) were found at 1.5 m from the patient in both groups, but that obviously a greater concentration was at 0.4m. Common sense: the further from the source of potential aerosol source the better.
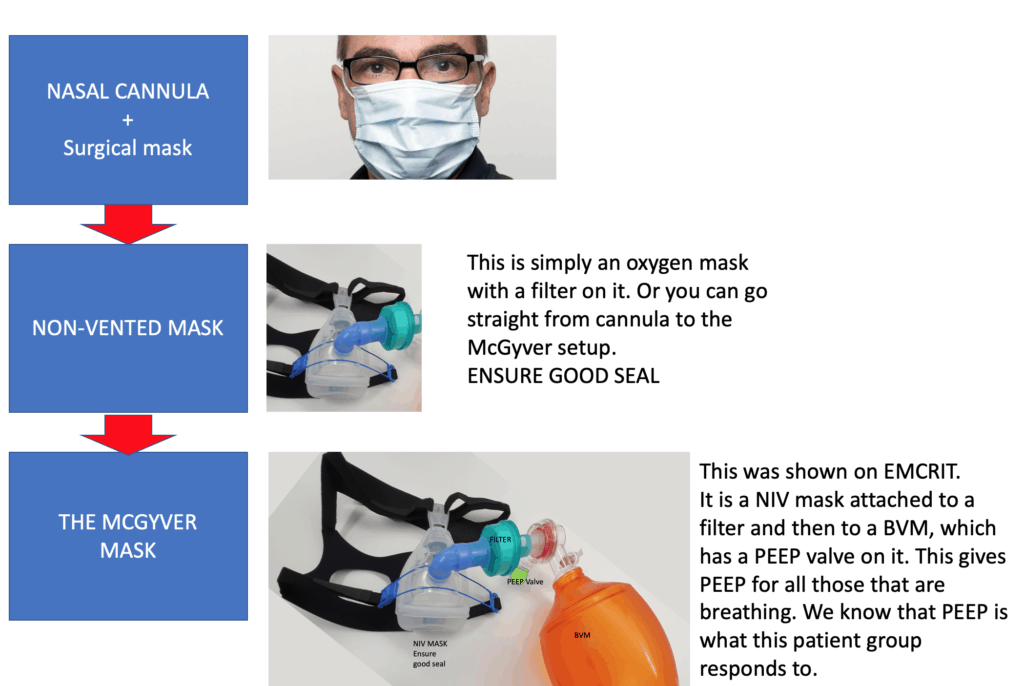
- Try to use non-vented systems so that there is no expulsion of aerosol laterally through the mask

Perhaps a non-vented mask with a filter attached to oxygen is the alternative.
I will probably be moving from nasal cannula to the more aggressive setup that gives PEEP as shown below:

Are there any studies you know that can help? List them below.
References
- Hui DSC et al. Aerosol dispersion during various respiratory therapies: A risk assessment model of nosocomial infection to healthcare workers. Hong Kong Med J 2014;20(Supplt)S9-13.
- Somogyi R et al Dispersal of Respiratory Droplets With Open vs Closed Oxygen Delivery Masks. Implications for the Transmission of Severe Acute Respiratory Syndrome. CHEST 2004; 125:1155–1157
- Leung CCH et al. Comparison of high-flow nasal cannula versus oxygen face mask for environmental bacterial contamination in critically ill pneumonia patients: a randomized controlled crossover trial. Journal of Hospital Infection 101 (2019) 84e87
- Scott Weingart. COVID Airway Management Thoughts. EMCrit Blog. Published on March 27, 2020. Accessed on April 3rd 2020. Available at [https://emcrit.org/emcrit/covid-airway-management/ ].


