
What if we had a way to predict PEA/Asystolic Cardiac Arrest, a few minutes before it happened? Would that be helpful?…. Perhaps.
PEA and asystolic cardiac arrests have a very poor outcome. The rate of survival in out of hospital arrests is less than 2%. In hospital, survival is higher, at about 30%(1).
Having this knowledge may or may not change the outcome, but I think it gives us a significant advantage, at least in our mental preparation.
In a recent research paper by Do et al in Resuscitation(2), they identified a right ventricular strain pattern that preceded hypoxic pulseless electrical activity cardiac arrest.
STUDY DESIGN: What they did.
This was a retrospective cross sectional study at two tertiary care hospitals. They looked at in hospital cardiac arrests due to PEA/Asystole
- Patients were at least 18 years of age
- There was telemetry data for at least 3 hours prior to the arrest.
- n=140
Patients were excluded if they had:
- pulmonary hypertension
- right ventricular enlargement on ECG,
- ventricular paced rhythm,
- an out of hospital arrest leading to the current admission,
- this was not their first in hospital cardiac arrest.
Right Ventricular strain pattern
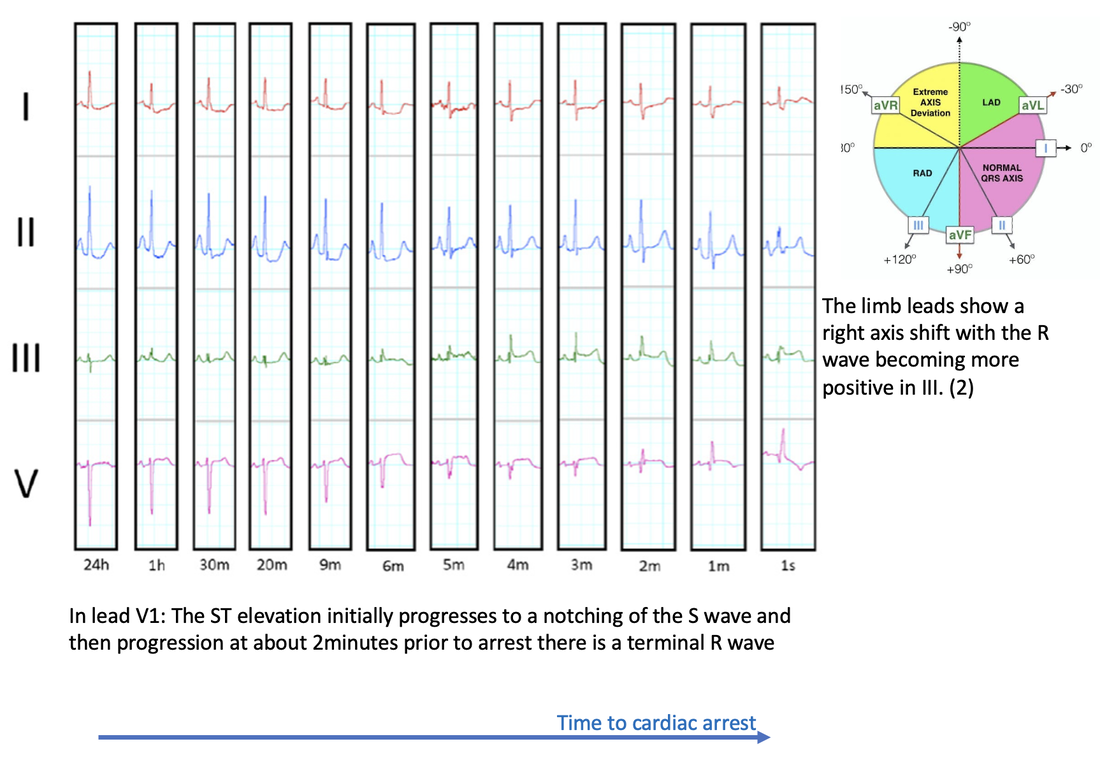
The most common terminal morphology(67% of cases) was a RBBB in V1, which progressed from an increasing RV delay as shown below:

Definite Right Ventricular strain(RVS) pattern was defined as having the above progressive morphological changes in lead V1 and either no intraventricular conduction delay or terminal intraventricular conduction delay (ie., incomplete RBBB) and two or more of the following occurring simultaneously:
- ST elevation V1
- Rightward directed ST elevation vector in limb leads (i.e. towards lead III) or
- Right axis deviation in limb leads
Possible RVS was defined as the RV delay pattern in V1 and only one of the supporting features.
Results
- The median time of RVS pattern to appear on the ECG in those that had a previously normal baseline was 7.2 minutes before arrest.
- The RVS pattern prior to PEA/Asystolic arrest was present in 47% of patients, without pre-existing right ventricular hypertrophy
- In those patients with RVS pattern who went on to have a cardiac arrest and then ROSC, there was a 41% incidence of RV dysfunction on echo.
ECG Patterns identified
Conclusion
Next time we are monitoring a patient and see the gradual Right ventricular delay pattern, indicative of right ventricular failure, we should get ready as up to about half of these patients may have a PEA/Asystolic arrest in the next few minutes.
REFERENCES
- Holmberg Mathias J et al. Annual incidence of adult and paediatric in-hospital cardiac arrest in the United States. Circ Cardiovasc Qual Outcomes 2019; 12:e005580.
- Do D H. et al. Electrocardiographic right ventricular strain precedes hypoxic pulseless electrical activity cardiac arrests; Looking beyond pulmonary embolism. Resuscitation151(2020) pp 127-134.


